

Evaluating Endoscopic Retrograde Cholangiopancreatography (ERCP) Outcomes in the Management of Common Bile Duct Stones With a Focus on Difficult Stones: A Retrospective Single-Center Study on Bile Duct Navigation From Kashmir, North India
- PMID: 40734873
- PMCID: PMC12306517
- DOI: 10.7759/cureus.86956
Evaluating Endoscopic Retrograde Cholangiopancreatography (ERCP) Outcomes in the Management of Common Bile Duct Stones With a Focus on Difficult Stones: A Retrospective Single-Center Study on Bile Duct Navigation From Kashmir, North India
Abstract
Background: Biliary tract diseases place a significant burden on healthcare in Kashmir. Endoscopic retrograde cholangiopancreatography (ERCP) is the gold standard for managing common bile duct stones (CBDS). However, challenging CBDS present considerable obstacles and complicate patient care, highlighting the necessity for specialized expertise and collaborative approaches. This study evaluates the effectiveness and safety of ERCP in treating CBDS, particularly focusing on difficult-to-manage cases, at a tertiary care center in the Kashmir region of North India. Objective: This study aimed to investigate the therapeutic outcomes and safety profile of ERCP in CBDS management, emphasizing exploring optimal strategies and modalities for successfully removing complex and difficult-to-treat stones. Methods: A retrospective study was conducted on ERCPs performed between March 2024 and March 2025 at Sher-i-Kashmir Institute of Medical Sciences (SKIMS) in Srinagar, Kashmir, India. The efficacy of ERCP in clearing CBDS was assessed, and complications were noted. Patients with large (≥1.5 cm) stones of difficult morphology, such as barrel or square-shaped, or those with hard consistency, or those associated with stricture/narrowing seen on prior imaging or cholangiogram were classified as having "difficult" stones. A retrospective review of medical records analyzed patients with CBDS who underwent ERCP, evaluating procedure success, complications, and outcomes, with a focus on effectiveness in difficult CBD.
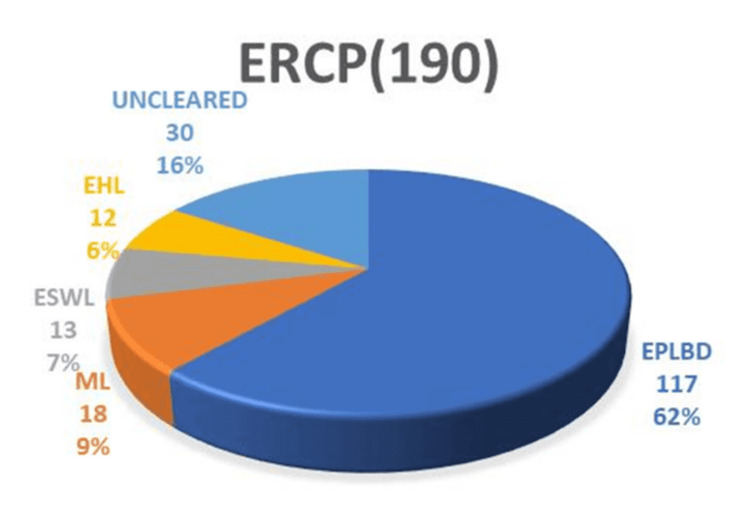
Results: The study achieved an overall CBDS clearance rate of 650/682 (95.3%), with a clearance rate of 160/190 (84.2%) for difficult stones. For difficult stones, endoscopic papillary large balloon dilation (EPLBD) alone was successful in 117/190 (61.5%) cases. Additional interventions, including mechanical lithotripsy (ML) in 18/190 (9.4%) cases, extracorporeal shock wave lithotripsy (ESWL) in 13/190 (6.8%) cases, and electrohydraulic lithotripsy (EHL) in 12/190 (6.3%) cases, were required. The overall success rates for these interventions were as follows: EPLBD 117/175 (66.8%), ML 18/30 (60%), ESWL 13/20 (65%), and EHL 12/13 (92.3%). Surgical intervention was required in 30/190 (15.7%) cases. Complications occurred in 82 (12%) of overall cases and 13 (6.8%) of difficult stone cases.
Conclusion: In conclusion, our findings underscore the value of ERCP in managing CBDS, particularly challenging ones, with high efficacy and an acceptable safety profile. This supports its continued use as a primary treatment option for complex CBDS. While complications related to ERCP do occur, they are primarily associated with sphincterotomy/precut procedures for gaining access to the CBD. Notably, managing difficult stones does not appear to increase the complication rate, further strengthening ERCP's role in the treatment of complex biliary cases.
Keywords: common bile duct stones (cbds); difficult cbd stone; electrohydraulic (ehl); endoscopic papillary large balloon dilation (eplbd); endoscopic retrograde cholangiopancreatography (ercp); mechanical lithotripsy (ml).
Copyright © 2025, Nazir et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Updated guideline on the management of common bile duct stones (CBDS) Williams E, Beckingham I, El Sayed G, Gurusamy K, Sturgess R, Webster G, Young T. Gut. 2017;66:765–782. - PubMed
-
- Optimizing choledocholithiasis management: a cost-effectiveness analysis. Poulose BK, Speroff T, Holzman MD. Arch Surg. 2007;142:43–48. - PubMed
-
- To study the safety and efficacy of ERCP and biliary stenting in the management of difficult common bile duct (CBD) stones in elderly patients. Ahmad SS, Akhter S, Altaf SH. https://academicmed.org/Uploads/Volume5Issue2/357.%20[372.%20JAMP_Yadav_... Int J Acad Med Pharm. 2023;5:1712–1716.
LinkOut - more resources
Full Text Sources