

Incidence of Acute Kidney Injury in Critically Ill Patients Receiving Vancomycin With Concomitant Piperacillin-Tazobactam Versus Other Beta-Lactams: A Systematic Review and Meta-Analysis
- PMID: 40735055
- PMCID: PMC12301226
- DOI: 10.1177/87551225251350894
Incidence of Acute Kidney Injury in Critically Ill Patients Receiving Vancomycin With Concomitant Piperacillin-Tazobactam Versus Other Beta-Lactams: A Systematic Review and Meta-Analysis
Abstract
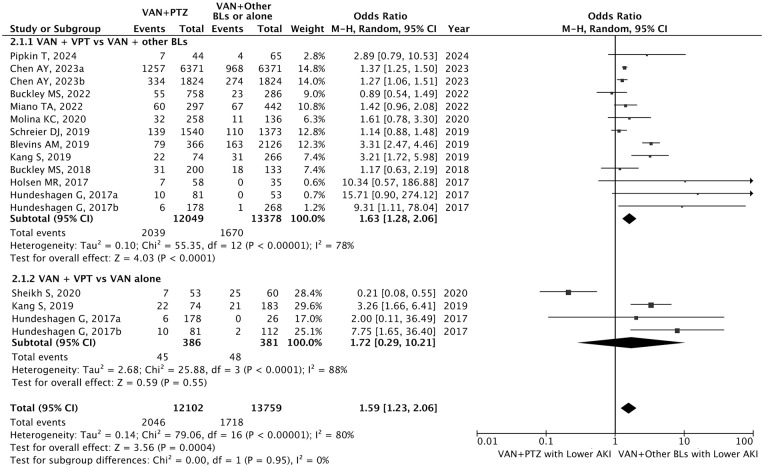
Objectives: To explore whether vancomycin (VAN) plus piperacillin-tazobactam (PTZ) was associated with an increased risk of acute kidney injury (AKI) compared with VAN plus other beta-lactams (BLs) or monotherapy in critically ill patients, where the evidence remains controversial. Data sources: PubMed, Cochrane, Web of Science, and Embase were searched from inception to June 2024. Study selection: Studies comparing the risk of AKI with one group receiving VAN+PTZ, and other groups receiving VAN plus other BLs, or monotherapy in critically ill. Data synthesis: This analysis included 20 articles with 28 243 participants. The majority of included studies were retrospective (95%, 19/20) and had moderate risks of bias (80.0%, 16/20). The results indicated VAN+PTZ was associated with a significantly higher risk of AKI compared with VAN plus other BLs (OR = 1.66, 95% CI = 1.42-1.94, P < 0.001). Subgroup analyses showed that compared with adults, children were associated with a higher risk of AKI when receiving VAN+PTZ (OR = 3.16 vs 1.59). Also, VAN+PTZ was associated with a significantly higher risk of severe stage 2 to 3 AKI than VAN plus other BLs (OR = 1.63, 95% CI = 1.28-2.06, P < 0.001). No significant difference was identified in mortality, dialysis, time to AKI, and length of stay between patients receiving VAN plus PTZ and other combinations. Conclusions: In critically ill, VAN plus PTZ was associated with an increased risk of AKI and severe stage 2 to 3 AKI compared with VAN plus other BLs, especially in children. However, more high-quality multicenter, prospective cohort studies, and randomized controlled studies are needed.
Keywords: acute kidney injury; beta-lactams; critically ill; piperacillin-tazobactam; vancomycin.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources