

Uraemic burden index: a novel predictor of pre-emptive kidney transplant outcome
- PMID: 40735146
- PMCID: PMC12304882
- DOI: 10.1093/ckj/sfaf129
Uraemic burden index: a novel predictor of pre-emptive kidney transplant outcome
Abstract
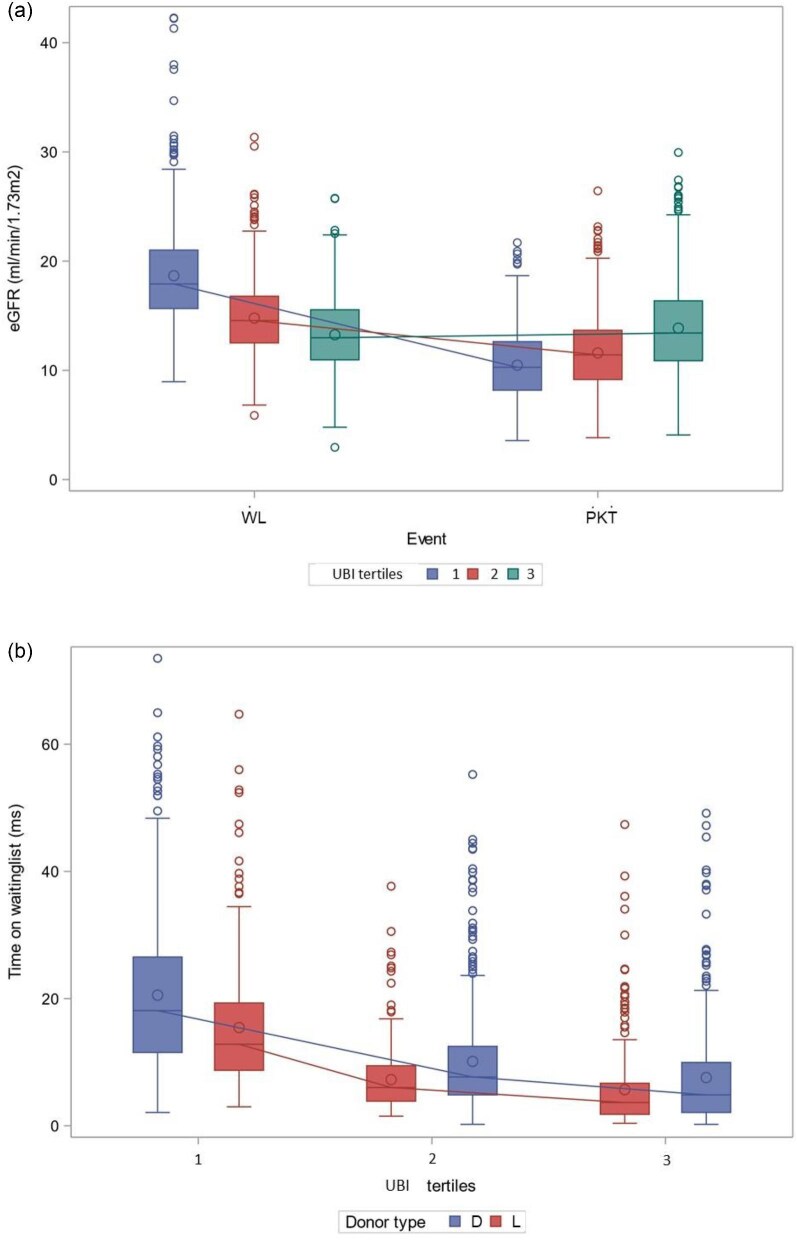
Timing of pre-emptive kidney transplantation (PKT) and the role of estimated glomerular filtration rate (eGFR) change in outcome prediction remains a subject of debate. This study aimed to assess potential factors, with special attention to uraemic burden, which may be associated with 5-year outcomes. In our retrospective observational cohort study, first PKT adults registered in the CRISTAL database between 2013 and 2019 were analysed to elucidate the role of eGFR and other associating factors with death and graft loss. Recipient-, donor- and transplantation-related features were analysed by using multivariable logistic regression analysis. A conditional inference tree was applied for risk stratification. A total of 2327 first PKT [52.8 years (interquartile range 43-64), 38% female) were included. The mean percentage of PKT over time was 14%. Primary kidney disease (congenital anomalies, glomerulonephritis and other causes versus autosomal dominant polycystic kidney disease), donor age and number of DR mismatches associated with combined 5-year outcomes [odds ratio 2.64 (95% confidence interval 1.42-4.93); 1.94 (1.1-4.93); 1.76 (1.06-2.92); 1.03 (1.02-1.05); 1.67 (1.1-2.53); P < .05], whereas donor type was not associated with outcomes. By supervised decision-tree analysis, >30% risk of failure in PKT was attributed to high recipient risk, higher donor age, uraemic burden index (UBI)-a novel parameter defined by the product of eGFR change and the logarithmic time on the waiting list-and two DR mismatches. In conclusion, eGFR and donor type were not associated with death or graft failure in PKT. UBI can potentially be a novel parameter of uraemic burden and contribute to predict 5-year risk of failure. Clinical decisions based on objective risk estimations might be crucial to approach the 'PKT in due course' concept.
Keywords: biomarker; eGFR; kidney transplantation; outcome; pre-emptive.
© The Author(s) 2025. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
O.C. is a member of the CKJ Editorial Board.
Figures






Similar articles
-
Sex and gender as predictors for allograft and patient-relevant outcomes after kidney transplantation.Cochrane Database Syst Rev. 2024 Dec 19;12(12):CD014966. doi: 10.1002/14651858.CD014966.pub2. Cochrane Database Syst Rev. 2024. PMID: 39698949
-
The experiences of adults who are on dialysis and waiting for a renal transplant from a deceased donor: a systematic review.JBI Database System Rev Implement Rep. 2015 Mar 12;13(2):169-211. doi: 10.11124/jbisrir-2015-1973. JBI Database System Rev Implement Rep. 2015. PMID: 26447040
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Normothermic and hypothermic machine perfusion preservation versus static cold storage for deceased donor kidney transplantation.Cochrane Database Syst Rev. 2024 Jul 9;7(7):CD011671. doi: 10.1002/14651858.CD011671.pub3. Cochrane Database Syst Rev. 2024. PMID: 38979743 Free PMC article.
-
Home versus in-centre haemodialysis for people with kidney failure.Cochrane Database Syst Rev. 2024 Apr 8;4(4):CD009535. doi: 10.1002/14651858.CD009535.pub3. Cochrane Database Syst Rev. 2024. PMID: 38588450 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
