

Risk factors for severe maternal morbidity in patients with hypertensive disorder of pregnancy: A retrospective study
- PMID: 40735566
- PMCID: PMC12302110
- DOI: 10.12669/pjms.41.7.12023
Risk factors for severe maternal morbidity in patients with hypertensive disorder of pregnancy: A retrospective study
Abstract
Objective: To identify significant risk factors associated with severe maternal morbidity(SMM) in patients with hypertensive disorder of pregnancy (HDP).
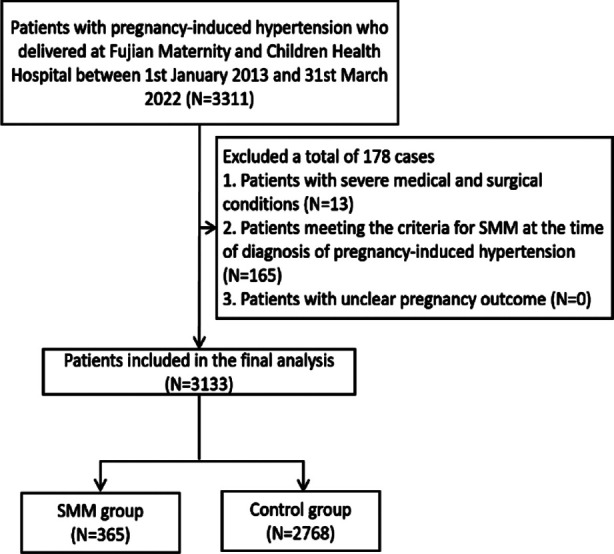
Methods: This retrospective study analyzed clinical data from patients with HDP who delivered at Fujian Maternity and Children Health Hospital between January 2013 and March 2022. Univariate logistic regression analysis was performed to identify risk factors for developing SMM. Significant risk factors (P < 0.05) were considered for inclusion in multivariate logistic regression using stepwise regression with forward and backward selection.
Results: Of 3133 HDP patients included in the study, 365 met the diagnostic criteria of SMM and were included in the SMM group, while 2768 patients comprised the control group. The SMM group had a significantly higher incidence of gestational hypertension diagnosed at ≤ 34 weeks of gestation compared to the control group (30.14% vs. 12.64%, p<0.0001). Patients in the SMM group had a higher incidence of previous history of preeclampsia compared to the control group (1.64% vs. 0.25%, p=0.0001). Logistic regression analysis identified parity (OR, 1.37; CI, 1.05-1.78; p=0.0205), gestational age of diagnosis (OR, 2.22; CI, 1.68-2.92; p<0.0001), iron supplementation (OR, 2.31; CI, 1.83-2.93; p<0.0001), and preeclampsia (OR, 3.10; CI, 2.42-3.98; p<0.0001) as significant risk factors for SMM. Stepwise regression analysis confirmed that parity (OR, 1.43; CI, 1.17-1.73; p=0.0004), gestational age of diagnosis (OR, 2.32; CI, 1.77-3.05; p<0.0001), iron supplementation (OR, 2.30; CI, 1.82-2.90; p<0.0001), and preeclampsia (OR, 3.34; CI, 2.63-4.24; p<0.0001) remained significantly associated with SMM.
Conclusion: Gestational age of diagnosis, iron supplementation, and history of preeclampsia were identified as risk factors of SMM in patients with HDP. Our results can help identify high-risk patients for early recognition and management of SMM.
Keywords: Hypertensive disorder of pregnancy; Iron supplementation; Preeclampsia; Risk factors; Severe maternal morbidity.
Copyright: © Pakistan Journal of Medical Sciences.
Figures
Similar articles
-
Severe Maternal Morbidity Associated With Chronic Hypertension, Preeclampsia, and Gestational Hypertension.JAMA Netw Open. 2025 Jan 2;8(1):e2451406. doi: 10.1001/jamanetworkopen.2024.51406. JAMA Netw Open. 2025. PMID: 39874039 Free PMC article.
-
The Association of Race and Ethnicity with Severe Maternal Morbidity among Individuals Diagnosed with Hypertensive Disorders of Pregnancy.Am J Perinatol. 2023 Apr;40(5):453-460. doi: 10.1055/a-1886-5404. Epub 2022 Jun 28. Am J Perinatol. 2023. PMID: 35764308 Free PMC article.
-
Planned early delivery versus expectant management for hypertensive disorders from 34 weeks gestation to term.Cochrane Database Syst Rev. 2017 Jan 15;1(1):CD009273. doi: 10.1002/14651858.CD009273.pub2. Cochrane Database Syst Rev. 2017. PMID: 28106904 Free PMC article.
-
Maternal and neonatal outcomes of elective induction of labor.Evid Rep Technol Assess (Full Rep). 2009 Mar;(176):1-257. Evid Rep Technol Assess (Full Rep). 2009. PMID: 19408970 Free PMC article.
-
Antenatal dietary supplementation with myo-inositol in women during pregnancy for preventing gestational diabetes.Cochrane Database Syst Rev. 2015 Dec 17;2015(12):CD011507. doi: 10.1002/14651858.CD011507.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2023 Feb 15;2:CD011507. doi: 10.1002/14651858.CD011507.pub3. PMID: 26678256 Free PMC article. Updated.
References
-
- Garovic VD, Dechend R, Easterling T, Karumanchi SA, McMurtry Baird S, Magee LA, et al. Hypertension in Pregnancy:Diagnosis, Blood Pressure Goals, and Pharmacotherapy:A Scientific Statement From the American Heart Association. Hypertension. 2022;79(2):e21–e41. doi:10.1161/HYP.0000000000000208. - PMC - PubMed
-
- Ananth CV, Vintzileos AM. Maternal-fetal conditions necessitating a medical intervention resulting in preterm birth. Am J Obstet Gynecol. 2006;195(6):1557–1563. doi:10.1016/j.ajog.2006.05.021. - PubMed
-
- Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol. 2009;33(3):130–137. doi:10.1053/j.semperi.2009.02.010. - PubMed
-
- Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP, Saito S, et al. The hypertensive disorders of pregnancy:ISSHP classification, diagnosis &management recommendations for international practice. Pregnancy Hypertens. 2018;13:291–310. doi:10.1016/j.preghy.2018.05.004. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous