

The diagnostic utility of lung ultrasound in the assessment of interstitial lung disease associated with rheumatoid arthritis
- PMID: 40739275
- PMCID: PMC12309050
- DOI: 10.1186/s13075-025-03626-4
The diagnostic utility of lung ultrasound in the assessment of interstitial lung disease associated with rheumatoid arthritis
Abstract
Background: To investigate the diagnostic accuracy of lung ultrasound (LUS) for interstitial lung disease (ILD) in patients with rheumatoid arthritis (RA).
Methods: This retrospective study included patients over 18 years with RA evaluated at the Department of Rheumatology and Immunology of Shantou Central Hospital. All patients underwent chest high-resolution computed tomography (HRCT) and LUS within one month. The LUS was performed in a total of 50 scanning sites (ScS), and the number of B-lines present in each ScS was counted and summed up as B-lines score. A positive judgement was given on LUS when the B-lines score exceeded 10. The presence and patterns of ILD were defined by HRCT findings. ROC curve analysis was used to calculate the accuracy of LUS to detect ILD.
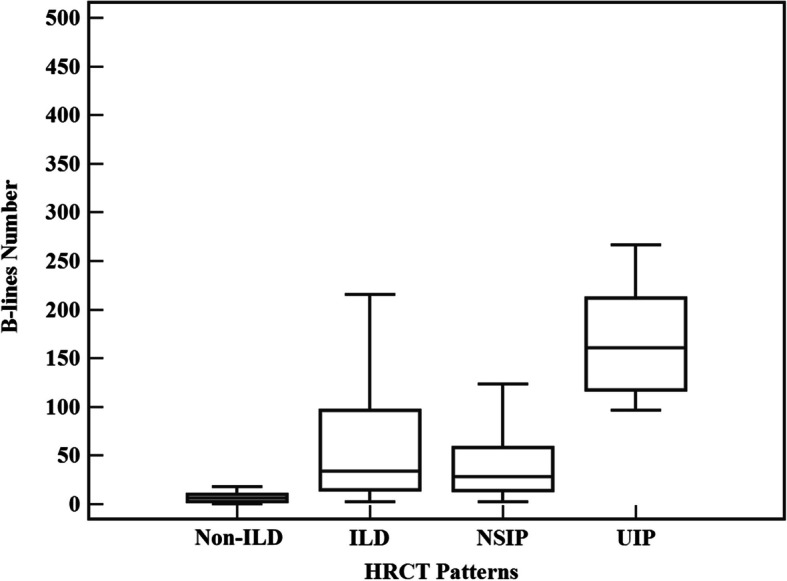
Results: A total of 120 RA patients (86 women, with a median age of 56.0 [50.0-64.0] years) were enrolled. Based on the HRCT, 76 patients were found to have radiographic ILD, with 63 exhibiting nonspecific interstitial pneumonia (NSIP) and 13 showing usual interstitial pneumonia (UIP). Sonographic ILD was detected in 76 patients who underwent LUS examination. The concordance rate between two modalities was 83.33% (Kappa value = 0.64, 95% CI 0.50-0.78). The diagnostic sensitivity and specificity of LUS were 86.84% and 77.27%, respectively. The positive predictive value, negative predictive value, a positive likelihood ratio and a negative likelihood ratio were 86.84%, 77.27%, 3.82, and 0.17, respectively. The number of B-lines in RA with ILD and without ILD on HRCT showed a significant difference (34.0 [15.0-96.5] vs. 6.5 [2.5-10.0], P < 0.001). The presence of 12 B-lines on 50 ScS was the optimal cutoff value for detecting RA-ILD (AUC = 0.89, 95% CI 0.82-0.94, sensitivity of 85.53%, specificity of 81.82%, P < 0.001).
Conclusions: Lung ultrasound is a valuable diagnostic tool for RA-ILD and can be used as a screening method to identify patients who require further evaluation with chest HRCT.
Keywords: B-lines; High-resolution computed tomography; Interstitial lung disease; Lung ultrasound; Rheumatoid arthritis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Shantou Central Hospital Ethics Committee (2024-KY-018). It was conducted by the principles of the Declaration of Helsinki. All patients signed the informed consents. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
Clinical variables and lung ultrasonography for the screening of interstitial lung disease in patients with rheumatoid arthritis.Clin Rheumatol. 2025 Aug;44(8):3167-3175. doi: 10.1007/s10067-025-07510-z. Epub 2025 Jun 24. Clin Rheumatol. 2025. PMID: 40555925
-
Computed tomography-based quantitative scoring system for rheumatoid arthritis-associated interstitial lung disease: a retrospective diagnostic accuracy study for progressive fibrosis detection.Clin Rheumatol. 2025 Jul;44(7):2669-2681. doi: 10.1007/s10067-025-07511-y. Epub 2025 Jun 9. Clin Rheumatol. 2025. PMID: 40488936 Free PMC article.
-
Evaluation of the coalescent lung ultrasound score in rheumatoid arthritis-associated interstitial lung disease.Clin Rheumatol. 2025 Sep;44(9):3459-3465. doi: 10.1007/s10067-025-07589-4. Epub 2025 Jul 24. Clin Rheumatol. 2025. PMID: 40707847
-
Lung ultrasound as a screening tool for interstitial lung disease in patients with rheumatoid arthritis: state of the art.Curr Opin Pulm Med. 2025 Sep 1;31(5):476-483. doi: 10.1097/MCP.0000000000001200. Epub 2025 Jul 11. Curr Opin Pulm Med. 2025. PMID: 40643573 Review.
-
Evaluating the role of lung ultrasound in the diagnosis of rheumatoid arthritis-interstitial lung disease.Expert Rev Clin Immunol. 2025 Aug;21(8):1019-1033. doi: 10.1080/1744666X.2025.2539440. Epub 2025 Jul 28. Expert Rev Clin Immunol. 2025. PMID: 40704486 Review.
References
-
- Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388(10055):2023–38. - PubMed
-
- Smolen JS, Aletaha D, Barton A, Burmester GR, Emery P, Firestein GS, et al. Rheumatoid arthritis Nat Rev Dis Primers. 2018;4:18001. - PubMed
-
- Lee EE, Shin A, Lee J, Lee JH, Ha YJ, Lee YJ, et al. All-cause and cause-specific mortality of patients with rheumatoid arthritis in Korea: A nation-wide population-based study. Joint Bone Spine. 2022;89(1): 105269. - PubMed
-
- Spagnolo P, Lee JS, Sverzellati N, Rossi G, Cottin V. The Lung in Rheumatoid Arthritis: Focus on Interstitial Lung Disease. Arthritis Rheumatol. 2018;70(10):1544–54. - PubMed
-
- Young A, Koduri G, Batley M, Kulinskaya E, Gough A, Norton S, et al. Mortality in rheumatoid arthritis. Increased in the early course of disease, in ischaemic heart disease and in pulmonary fibrosis. Rheumatology. 2007;46(2):350–357. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
