

Global inequities in the survival of extremely preterm infants: a systematic review and meta-analysis
- PMID: 40739629
- PMCID: PMC12309206
- DOI: 10.1186/s12887-025-05933-w
Global inequities in the survival of extremely preterm infants: a systematic review and meta-analysis
Abstract
Background: Despite the associated major morbidities, advances in neonatal care units have improved the survival rates of extremely preterm infants. However, the varying survival rates make it challenging to set policy decisions around the standardization of care. Therefore, this study aimed to determine the global survival rate of extremely preterm infants and to compare it across different income levels and over time during the last two decades.
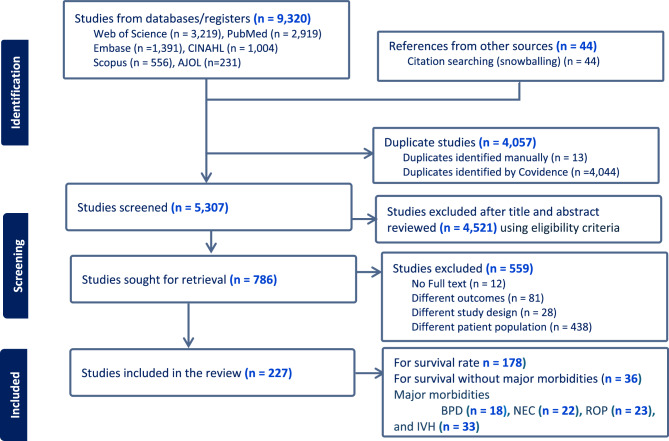
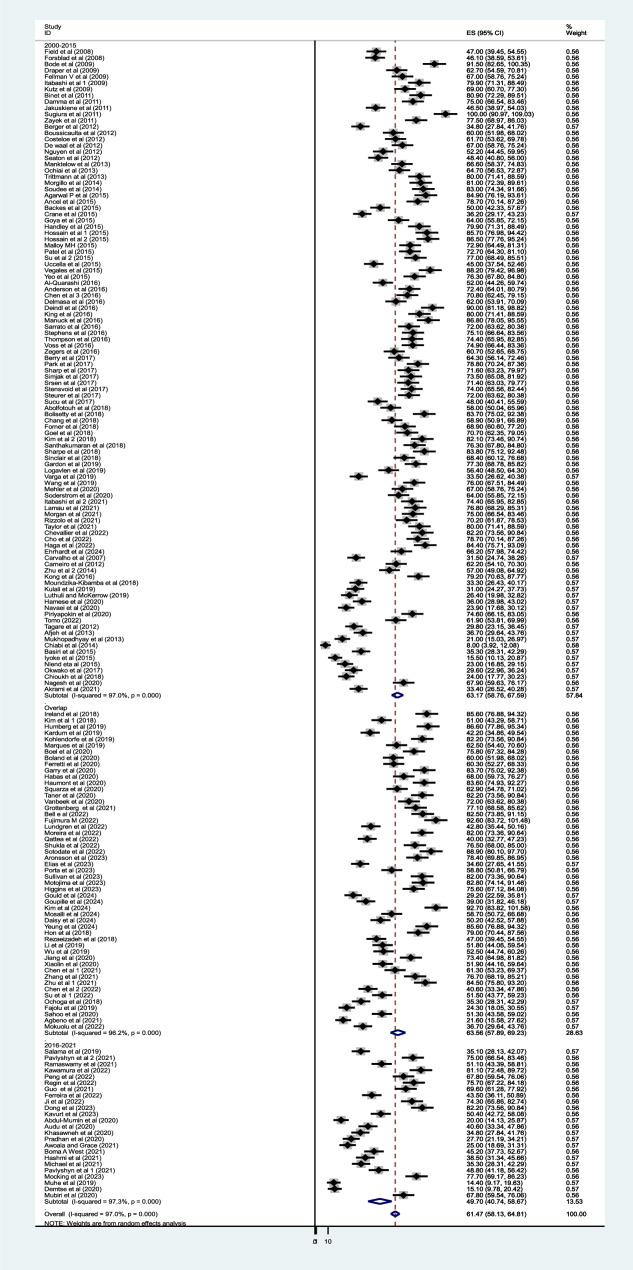
Method: A comprehensive systematic search was conducted across major databases, including PubMed/Medline, EMBASE, CINAHL, Web of Science, Scopus, AJOL, Google Scholar and Google, to identify relevant articles. All peer-reviewed studies reported the survival rate of extremely preterm infants (born before 29 weeks' gestation) between January 1st, 2000, and June 25th, 2024, were included. Outcomes were compared between Epoch 1 (2000-2015, Millennium Developmental Goals period) and Epoch 2 (2016-2024, Sustainable Developmental Goals period). DerSimonian‒Laird random effects model was fitted to estimate the pooled weighted outcomes.
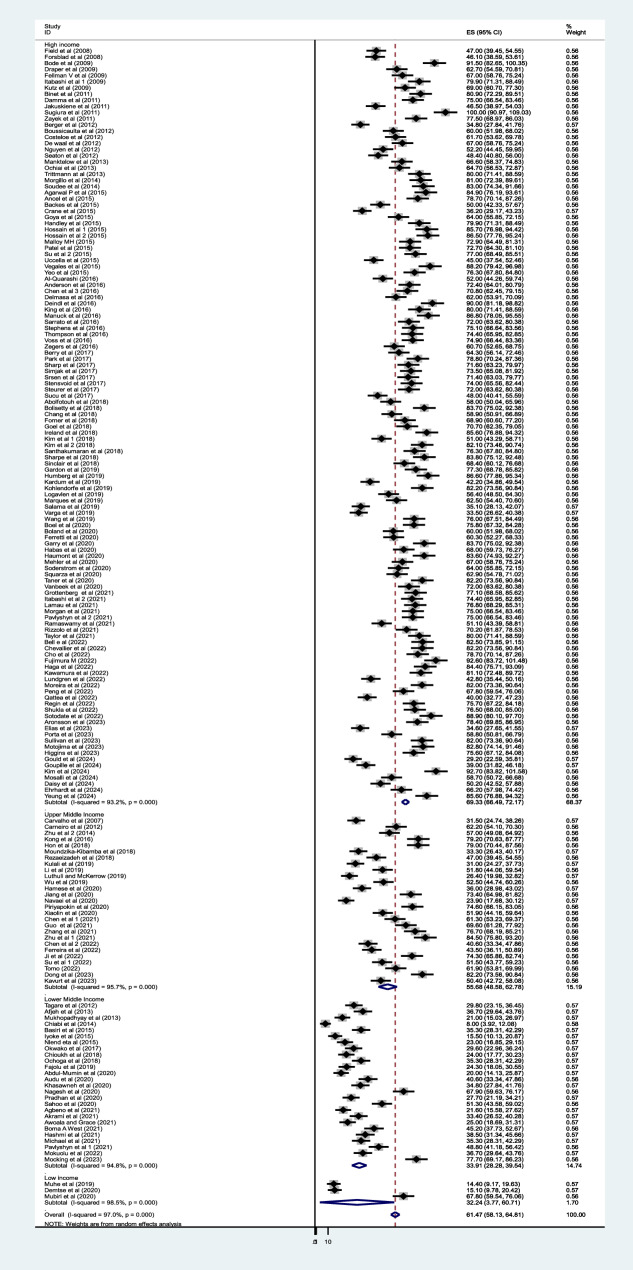
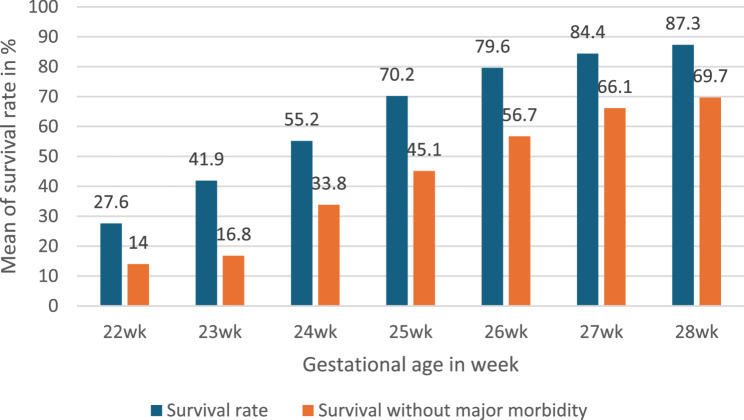
Results: A total of 217 studies involving 917,176 infants were included. Based on published data, 61.4% (95% CI: 58.13-64.81) of extremely preterm infants survived to discharge, and 51.7% (95% CI: 44.25-59.22) of survivors were discharged without major morbidity. Survival rate was significantly lower in low- and middle-income countries (44.3%) compared to high-income countries (69.3%). Among low- and middle-income countries, survival improved from 38% during the epoch 1 to 44.8% during the epoch 2. While in high-income countries it was 69.9% during epoch 1 and 64.2% during epoch 2. These findings are based on reported literature; may not fully reflect outcomes in low-resource settings where data are limited and underreported. Variability in the inclusion and care of borderline viable infants also contributes to the heterogeneity and uncertainty of the estimates.
Conclusion: Survival of extremely preterm infants varies widely across settings, with fewer than half surviving in low- and middle-income countries. While some improvement was observed in these regions during the Sustainable Developmental Goals period, comparisons across epochs and regions should be interpreted cautiously due to differences in data availability and population characteristics. These variations underscore the need for context-specific strategies that balance available resources, cultural values, and ethical considerations. Further population-level data, particularly from low-and middle-income countries, are essential to inform equitable global neonatal care policies.
Registration: PROSPERO (CDR42023447612 (PROSPERO (york.ac.uk)).
Clinical trial number: Not applicable.
Keywords: Extremely preterm infant; Meta-analysis; Survival rate.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Ohuma E, Moller A, Bradley E. National, regional, and worldwide estimates of preterm birth in 2020, with trends from 2010: A systematic analysis. Lancet. 2023. 10.1016/S0140-6736%2823%2900878-4. - PubMed
-
- Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385(9966):430–40. - PubMed
-
- Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–72. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
