

Left ventricular wall thickness heterogeneity improves cardiovascular disease diagnosis and prognosis: a UK Biobank cardiovascular magnetic resonance cohort study
- PMID: 40740418
- PMCID: PMC12308483
- DOI: 10.1093/ehjimp/qyaf092
Left ventricular wall thickness heterogeneity improves cardiovascular disease diagnosis and prognosis: a UK Biobank cardiovascular magnetic resonance cohort study
Abstract
Aims: Left ventricular hypertrophy (LVH) regionality carries diagnostic and prognostic importance. Mean absolute deviation of maximum segmental wall thickness (MadWT) is a novel left ventricular wall thickness (LVWT) heterogeneity biomarker from cardiovascular magnetic resonance imaging (CMR).
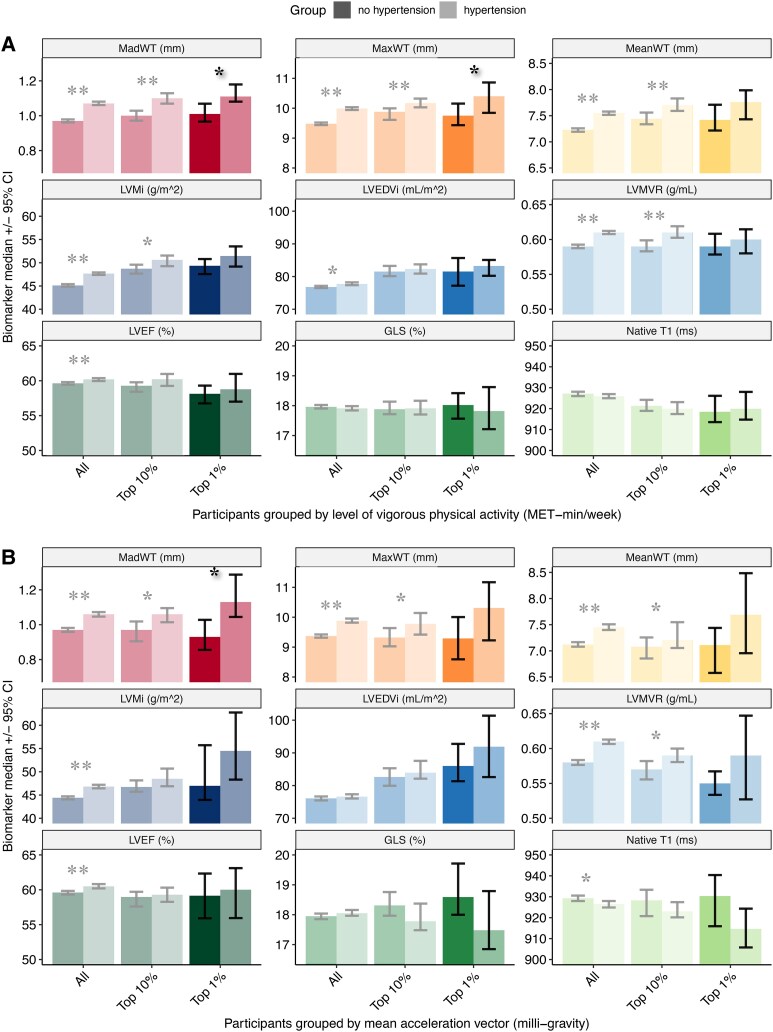
Objectives: To compare MadWT to indexed LV mass (LVMi), maximum (MaxWT) and mean (MeanWT) wall thickness to predict incident cardiovascular disease (CVD) and differentiate physiological from pathological LVH in highly physically active individuals.
Methods and results: Deep learning-assisted analysis of 44 930 UK Biobank CMR scans produced WT indices. Cox regression modelled major adverse cardiovascular events (MACE), heart failure (HF), arrhythmia, and all-cause death against LVWT indices. In the top 1% most physically active biomarker differences between propensity score matched hypertensive and non-hypertensive groups were compared. Over median (Q1, Q3) follow-up of 5.7 (4.9, 7.1) years, MadWT, MaxWT, MeanWT, and LVMi were associated with greater risk of MACE, HF, arrhythmia (P < 0.05), but not all-cause death (P > 0.05). After adjusting for CMR biomarkers, including LVMi, MadWT remained independently prognostic of the greatest number of endpoints, including MACE, HF, and arrhythmia [HR 1.13 (1.04-1.23); HR 1.15 (1.01-1.32); and HR 1.26 (1.18-1.35) respectively]. In the top 1% most physically active by three metrics, MadWT was the only significantly different biomarker between hypertensive and non-hypertensive participants (P < 0.05).
Conclusion: MadWT is important prognostically beyond LV mass and may be useful when differentiating physiological from hypertensive LVH. Although findings require confirmation in athletic and diseased cohorts, MadWT is readily translatable to deep learning-assisted clinical CMR reporting, especially in early unexplained LVH.
Keywords: biomarker; cardiovascular magnetic resonance imaging; heterogeneity; left ventricular hypertrophy; wall thickness.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: S.E.P. provides consultancy to Cardiovascular Imaging Inc, Calgary, Alberta, Canada. The remaining authors have nothing to disclose.
Figures



Similar articles
-
Diagnostic and prognostic value of ECG-predicted hypertension-mediated left ventricular hypertrophy using machine learning.J Hypertens. 2025 Aug 1;43(8):1327-1338. doi: 10.1097/HJH.0000000000004034. Epub 2025 May 23. J Hypertens. 2025. PMID: 40407114 Free PMC article.
-
Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Feb 24;2(2):CD013556. doi: 10.1002/14651858.CD013556.pub2. Cochrane Database Syst Rev. 2022. PMID: 35199850 Free PMC article.
-
Pharmacotherapy for hypertension-induced left ventricular hypertrophy.Cochrane Database Syst Rev. 2021 Oct 10;10(10):CD012039. doi: 10.1002/14651858.CD012039.pub3. Cochrane Database Syst Rev. 2021. PMID: 34628642 Free PMC article.
-
The comparative and added prognostic value of biomarkers to the Revised Cardiac Risk Index for preoperative prediction of major adverse cardiac events and all-cause mortality in patients who undergo noncardiac surgery.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD013139. doi: 10.1002/14651858.CD013139.pub2. Cochrane Database Syst Rev. 2021. PMID: 34931303 Free PMC article.
-
Smoking cessation for secondary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Aug 8;8(8):CD014936. doi: 10.1002/14651858.CD014936.pub2. Cochrane Database Syst Rev. 2022. PMID: 35938889 Free PMC article.
References
-
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Left ventricular mass and incidence of coronary heart disease in an elderly cohort. The Framingham Heart Study. Ann Intern Med 1989;110:101–7. - PubMed
-
- Kannel WB, Gordon T, Castelli WP, Margolis JR. Electrocardiographic left ventricular hypertrophy and risk of coronary heart disease. The Framingham study. Ann Intern Med 1970;72:813–22. - PubMed
-
- Moura B, Aimo A, Al-Mohammad A, Keramida K, Ben Gal T, Dorbala S et al. Diagnosis and management of patients with left ventricular hypertrophy: role of multimodality cardiac imaging. A scientific statement of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2023;25:1493–506. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous