

This is a preprint.
Predicting Neoadjuvant Chemotherapy Response in Triple-Negative Breast Cancer Using Pre-Treatment Histopathologic Images
- PMID: 40740511
- PMCID: PMC12310126
Predicting Neoadjuvant Chemotherapy Response in Triple-Negative Breast Cancer Using Pre-Treatment Histopathologic Images
Update in
-
Predicting Neoadjuvant Chemotherapy Response in Triple-Negative Breast Cancer Using Pre-Treatment Histopathologic Images.Cancers (Basel). 2025 Jul 22;17(15):2423. doi: 10.3390/cancers17152423. Cancers (Basel). 2025. PMID: 40805125 Free PMC article.
Abstract
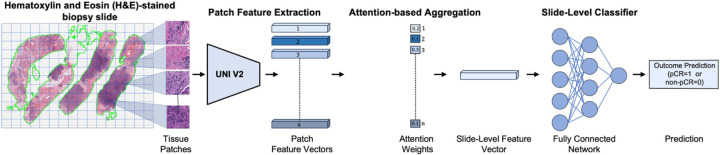
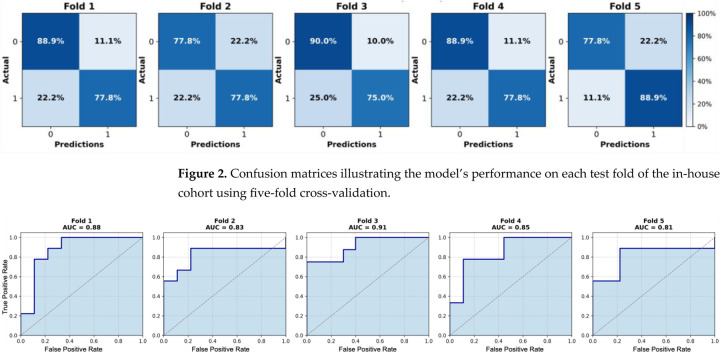
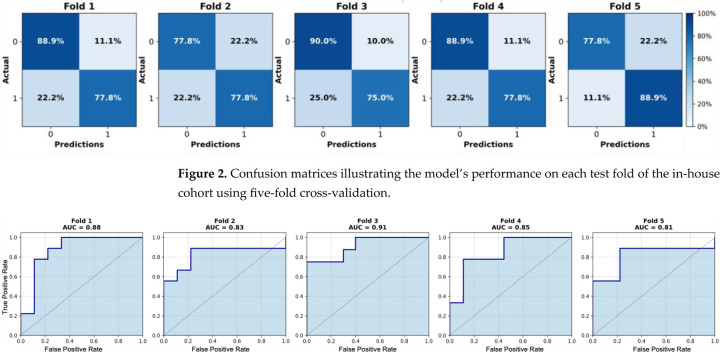
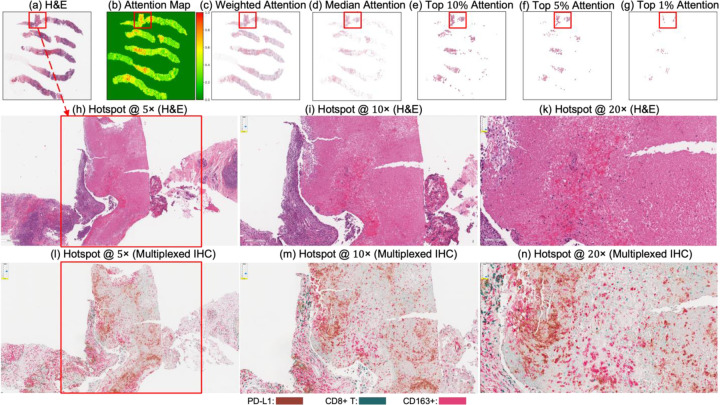
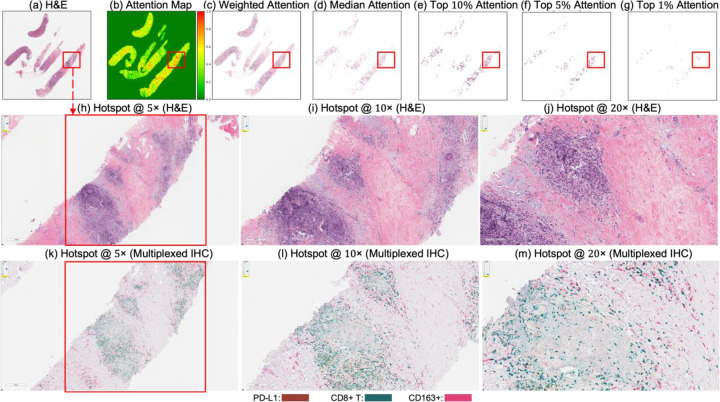
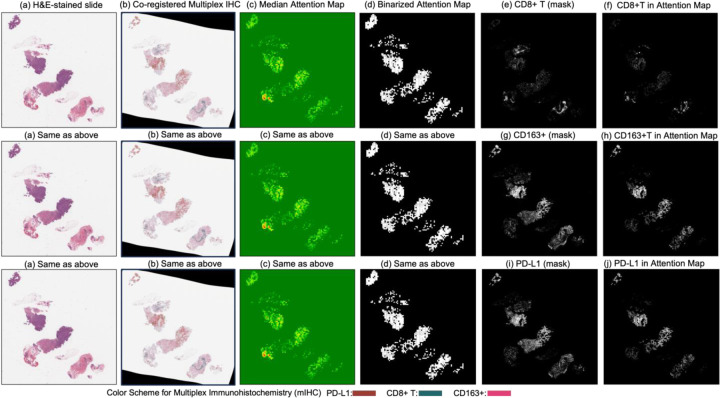
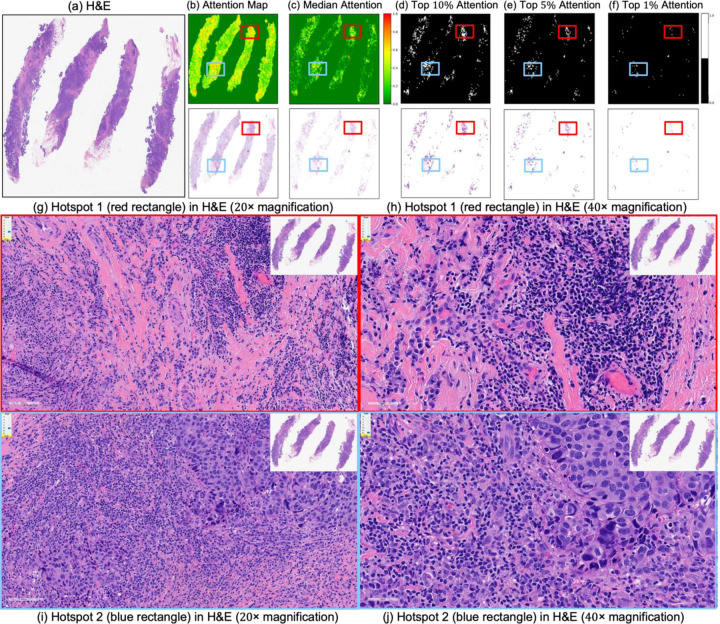
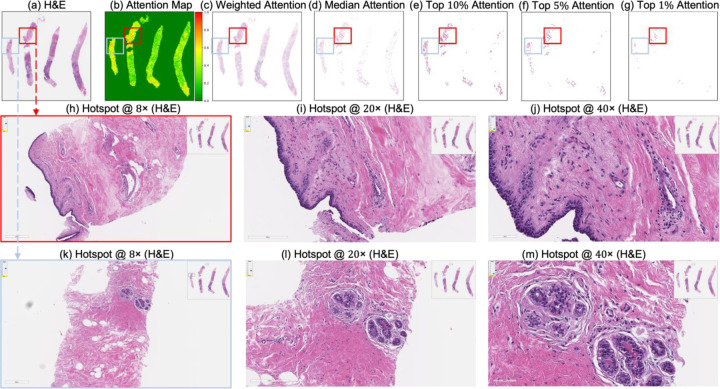
Triple-negative breast cancer (TNBC) remains a major clinical challenge due to its aggressive behavior and lack of targeted therapies. Accurate early prediction of response to neoadjuvant chemotherapy (NACT) is essential for guiding personalized treatment strategies and improving patient outcomes. In this study, we present an attention-based multiple instance learning (MIL) framework designed to predict pathologic complete response (pCR) directly from pre-treatment hematoxylin and eosin (H&E)-stained biopsy slides. The model was trained on a retrospective in-house cohort of 174 TNBC patients and externally validated on an independent cohort (n = 30). It achieved a mean area under the curve (AUC) of 0.85 during five-fold cross-validation and 0.78 on external testing, demonstrating robust predictive performance and generalizability. To enhance model interpretability, attention maps were spatially co-registered with multiplex immunohistochemistry (mIHC) data stained for PD-L1, CD8+ T cells, and CD163+ macrophages. The attention regions exhibited moderate spatial overlap with immune-enriched areas, with mean Intersection over Union (IoU) scores of 0.47 for PD-L1, 0.45 for CD8+ T cells, and 0.46 for CD163+ macrophages. The presence of these biomarkers in high-attention regions supports their biological relevance to NACT response in TNBC. This not only improves model interpretability but may also inform future efforts to identify clinically actionable histological biomarkers directly from H&E-stained biopsy slides, further supporting the utility of this approach for accurate NACT response prediction and advancing precision oncology in TNBC.
Keywords: artificial intelligence (AI); neoadjuvant chemotherapy (NACT); pathologic complete response (pCR); treatment response prediction; triple-negative breast cancer (TNBC).
Conflict of interest statement
Conflicts of Interest: All authors have no conflicts of interest.
Figures
Similar articles
-
Predicting Neoadjuvant Chemotherapy Response in Triple-Negative Breast Cancer Using Pre-Treatment Histopathologic Images.Cancers (Basel). 2025 Jul 22;17(15):2423. doi: 10.3390/cancers17152423. Cancers (Basel). 2025. PMID: 40805125 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Predictive Value of Excision Repair Cross Complementation Group 1 (ERCC1) by Immunohistochemistry for Determining Neoadjuvant Chemotherapy Response in Triple-Negative Breast Cancers.Breast J. 2025 Feb 18;2025:8410670. doi: 10.1155/tbj/8410670. eCollection 2025. Breast J. 2025. PMID: 40008380 Free PMC article.
-
Platinum-based chemotherapy for early triple-negative breast cancer.Cochrane Database Syst Rev. 2023 Sep 8;9(9):CD014805. doi: 10.1002/14651858.CD014805.pub2. Cochrane Database Syst Rev. 2023. PMID: 37681577 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
References
-
- Marra A.; Curigliano G. Adjuvant and neoadjuvant treatment of triple-negative breast cancer with chemotherapy. Cancer J. 2021, 27, 41–49. - PubMed
-
- Ferlay J.; Steliarova-Foucher E.; Lortet-Tieulent J.; Rosso S.; Coebergh J.-W.W.; Comber H.; Forman D.; Bray F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials