

FLAIR hyperintense cortical lesions in myelin oligodendrocyte glycoprotein-associated encephalitis with seizures in children: a retrospective single-center case series
- PMID: 40740785
- PMCID: PMC12307442
- DOI: 10.3389/fimmu.2025.1563481
FLAIR hyperintense cortical lesions in myelin oligodendrocyte glycoprotein-associated encephalitis with seizures in children: a retrospective single-center case series
Abstract
Background and purpose: In recent years, the number of case reports concerning fluid-attenuated inversion recovery (FLAIR) hyperintense cortical lesions in myelin oligodendrocyte glycoprotein (MOG) -associated encephalitis with seizures (FLAMES) has been gradually increasing. However, within the pediatric demographic, there remains a lack of related serial reports. This study was designed to characterize the clinical features and prognosis of FLAMES in pediatric patients.
Methods: We reviewed the medical records of children diagnosed with FLAMES from January 2019 to July 2024 and retrospectively analyzed their clinical manifestations, brain magnetic resonance imaging (MRI) findings, laboratory results, treatments, and outcomes.
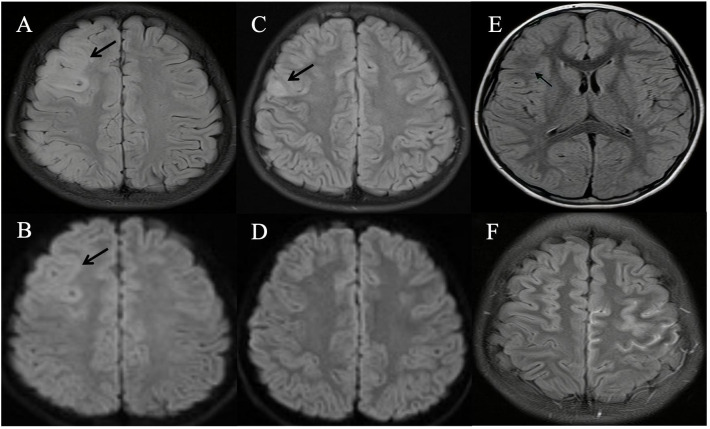
Results: Among the 123 children diagnosed with MOG antibody-associated diseases (MOGAD), 9 (7.3%) met the inclusion criteria for FLAMES. The median onset age was 9 years (range: 8-14), and the male-to-female ratio was 5:4. The most common clinical symptoms included seizures (9/9, with 6 experiencing focal seizures), altered mental status (6/9), headache (5/9), fever (4/9), and focal neurological deficits (3/9). Furthermore, three patients presented with status epilepticus, two with cranial nerve involvement (central facial paralysis and lingual paralysis), and two with Todd's palsy. Seven patients had cerebrospinal fluid (CSF) pleocytosis (median count: 58/µL, range: 12-143/µL); two had elevated CSF pressure (range: 240-280 mmH2O); and one had mildly elevated CSF protein levels (0.46 g/L). All patients had normal CSF glucose levels. Abnormal electroencephalogram (EEG) findings were detected in seven patients: epileptic seizures (3/7), interictal discharges (6/7), and slow background activity (3/7). Unilateral cortical hyperintense lesions were observed in all nine cases on FLAIR imaging of brain MRI, affecting the frontal (8/9), parietal (3/9), temporal (2/9), and occipital (1/9) lobes. Five patients exhibited distinct linear enhancement of the corresponding cerebral sulci and/or meninges on gadolinium-enhanced brain MRI. All patients received immunotherapy, and six were administered anti-seizure medicines (ASMs). Each child achieved a satisfactory outcome and remained relapse-free at the final follow-up.
Conclusion: FLAMES exhibit an age-dependent pattern. Epileptic seizures are the most common clinical symptom, with focal seizures being the predominant type. FLAIR-hyperintense cortical lesions typically present unilaterally, predominantly affecting the frontal lobes. Enhancement of the corresponding cerebral sulci and/or meninges may be a distinctive feature in children. For children with epilepsy, in the presence of recurrent seizures without identifiable triggers, especially when cortical lesions are detected in cranial MRI, consideration should be given to the possibility of FLAMES.
Keywords: brain magnetic resonance imaging; children; cortical encephalitis; myelin oligodendrocyte glycoprotein antibody; seizures.
Copyright © 2025 Liu, Wang, Jin, Chen, Wang, Liu and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical, imaging, and recurrence analysis of myelin oligodendrocyte glycoprotein antibody-associated disease with initial presentation as meningoencephalitis in children: a single-center retrospective study.Pediatr Radiol. 2025 Jun;55(7):1503-1514. doi: 10.1007/s00247-025-06269-4. Epub 2025 Jun 4. Pediatr Radiol. 2025. PMID: 40464908
-
Non-ADEM encephalitis in patients with myelin oligodendrocyte glycoprotein antibodies: a systematic review.Eur J Neurol. 2023 May;30(5):1515-1527. doi: 10.1111/ene.15684. Epub 2023 Feb 20. Eur J Neurol. 2023. PMID: 36704861
-
Clinical features of recurrent MOG antibody-associated cortical encephalitis in adults.Neurol Sci. 2025 May;46(5):1987-1993. doi: 10.1007/s10072-024-07978-8. Epub 2025 Jan 22. Neurol Sci. 2025. PMID: 39843649 Free PMC article.
-
Surgery for epilepsy.Cochrane Database Syst Rev. 2015 Jul 1;(7):CD010541. doi: 10.1002/14651858.CD010541.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2019 Jun 25;6:CD010541. doi: 10.1002/14651858.CD010541.pub3. PMID: 26130264 Updated.
-
Prognosis of adults and children following a first unprovoked seizure.Cochrane Database Syst Rev. 2023 Jan 23;1(1):CD013847. doi: 10.1002/14651858.CD013847.pub2. Cochrane Database Syst Rev. 2023. PMID: 36688481 Free PMC article.
References
-
- Höftberger R, Guo Y, Flanagan EP, Lopez-Chiriboga AS, Endmayr V, Hochmeister S, et al. The pathology of central nervous system inflammatory demyelinating disease accompanying myelin oligodendrocyte glycoprotein autoantibody. Acta Neuropathol. (2020) 139:875–92. doi: 10.1007/s00401-020-02132-y, PMID: - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous