

Sedation and analgesia doses do not differ across demographic factors in pediatric cardiac surgery patients
- PMID: 40740825
- PMCID: PMC12307295
- DOI: 10.3389/fped.2025.1577461
Sedation and analgesia doses do not differ across demographic factors in pediatric cardiac surgery patients
Abstract
Importance: Disparities in congenital heart disease, pediatric intensive care unit (ICU) outcomes, and acute pain control are common. The impact of patient race, ethnicity, and language on postoperative sedation and analgesia for pediatric patients undergoing cardiac surgery is unknown.
Objective: This study aims to investigate whether there are differences in sedation and analgesia in patients undergoing cardiac surgery according to patient race, ethnicity, and language in a study site that uses protocolized postoperative sedation and analgesia. We hypothesized that non-white and patients who prefer a language other than English would have differences in total doses of sedation compared with their white and English-speaking counterparts.
Design: This is a single-center, retrospective, observational cohort of pediatric patients admitted postoperatively to the cardiac ICU.
Setting: The study took place in an urban, quaternary, academic pediatric referral center.
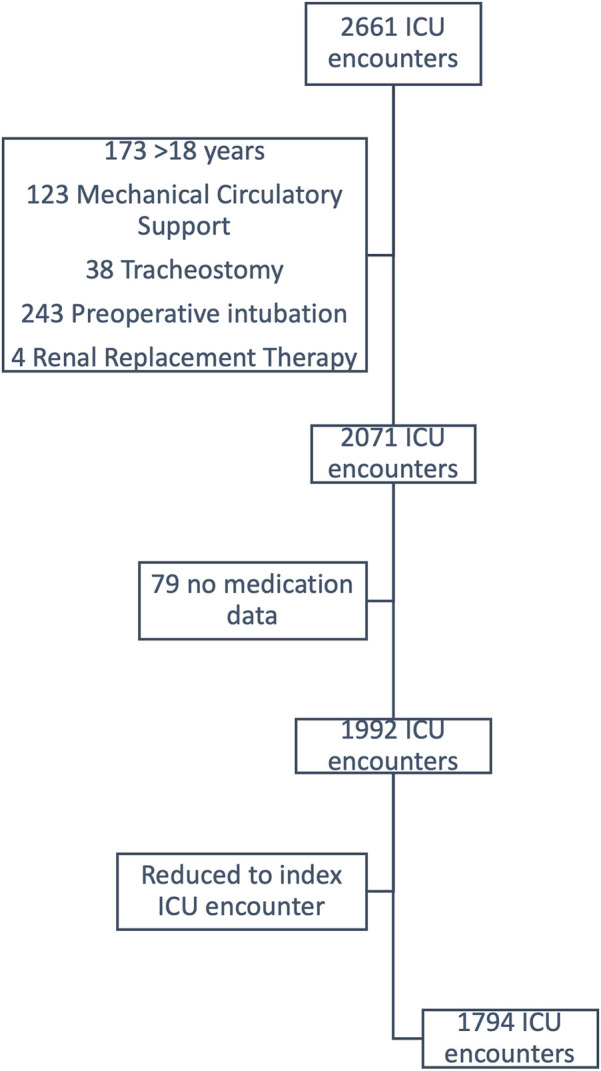
Participants: All pediatric patients, age 0-18 years, admitted to the cardiac ICU following their index cardiac surgery from 7/1/2018 to 6/30/2022 were included. Patients requiring renal replacement therapy, non-cardiac surgery during the same admission, tracheostomy, preoperative mechanical ventilation, or mechanical circulatory support prior to or following cardiac surgery were excluded.
Exposures: Exposure variables included patient race and ethnicity, preferred language, age, gender, Society of Thoracic Surgeons-European Association for Cardiothoracic Surgery category, use of cardiopulmonary bypass, duration of postoperative mechanical ventilation, and delayed sternal closure (DSC).
Main outcome and measure: The primary outcome was weight-adjusted doses of opioids in morphine equivalents, benzodiazepines in midazolam equivalents, and dexmedetomidine received in the first 72 h postoperatively.
Results: There were 1,794 postoperative admissions. 100% of patients received opioids, 42.5% received benzodiazepines, and 85% received dexmedetomidine. There were no differences in opioid, benzodiazepine, or dexmedetomidine doses according to patient race and ethnicity or preferred language. Patient race, ethnicity, and language were not associated with opioid or benzodiazepine dose in multivariable quantile regression. Multivariable regression for dexmedetomidine demonstrated similar results with age also being inversely correlated.
Conclusions: and Relevance: Doses of postoperative sedation and analgesia are not correlated with patient race, ethnicity, and language. Factors that were associated with differences in medication doses are reflective of postoperative acuity and are expected. Protocolized sedation and analgesia may be responsible for the lack of differences seen in this study when compared with other studies in similar settings. Future studies should compare protocolized and non-protocolized sedation and analgesia to further evaluate the protective effects of protocols against bias in clinical settings.
Keywords: analgesia & critical care; cardiac surgery; critical care; disparities health; sedation.
© 2025 Lawson, Achuff, Ankola, Guffey, Lopez and Afonso.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources