

Feasibility of single-port laparoscopic appendectomy for retrocecal appendicitis: A propensity score-matched study with multi-port laparoscopic appendectomy
- PMID: 40740912
- PMCID: PMC12305288
- DOI: 10.4240/wjgs.v17.i7.105925
Feasibility of single-port laparoscopic appendectomy for retrocecal appendicitis: A propensity score-matched study with multi-port laparoscopic appendectomy
Abstract
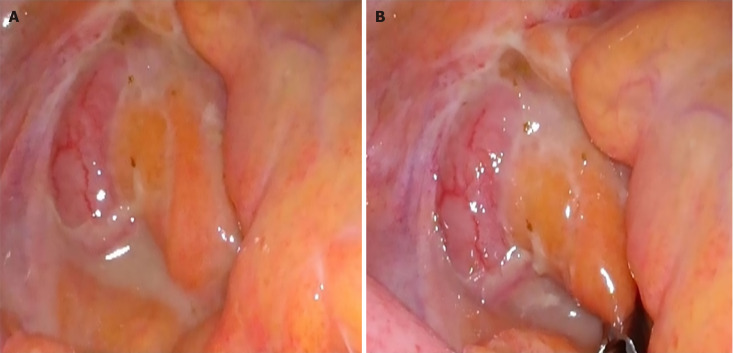
Background: Retrocecal appendicitis, the most common anatomical type, presents diagnostic and surgical challenges. Single-port laparoscopic appendectomy (SPLA) has been proposed as an alternative to multi-port laparoscopic appendectomy (MPLA) with advancements in minimally invasive surgery. However, few studies have compared the perioperative outcomes between the SPLA and MPLA for retrocecal appendicitis.
Aim: To compare the efficacy and safety between the SPLA and MPLA in treating retrocecal appendicitis, focusing on perioperative outcomes.
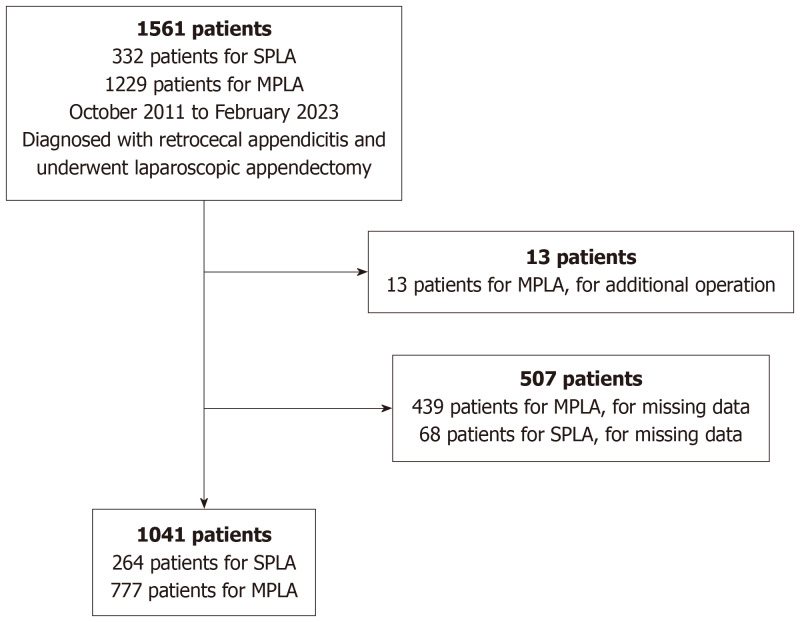
Methods: This retrospective study analyzed data from 1041 patients who underwent SPLA or MPLA at Konyang University Hospital between October 2011 and February 2023. Propensity score matching (PSM) was used to minimize selection bias, resulting in 235 patients in each group. Additionally, non-inferiority tests, post-hoc analysis, and multivariable regression analysis were performed to validate the results and assess factors affecting postoperative outcomes.
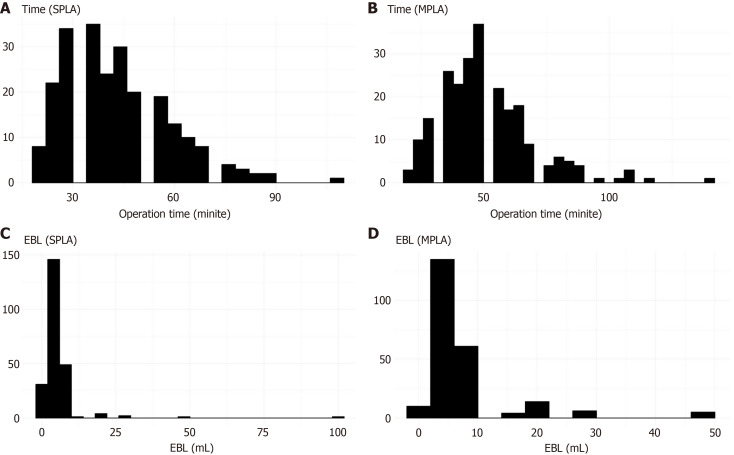
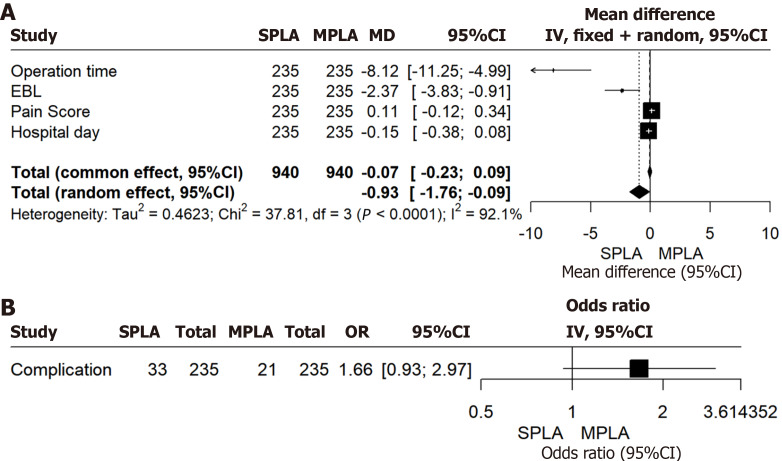
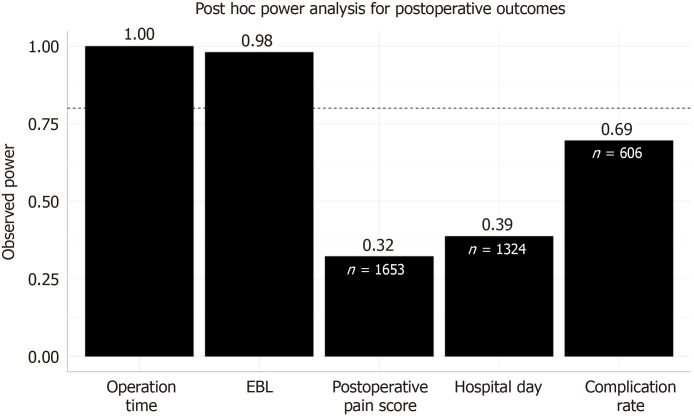
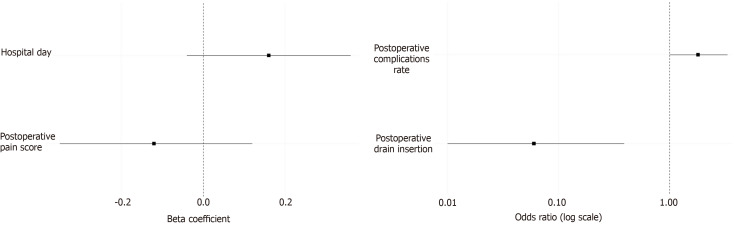
Results: After PSM, SPLA showed shorter operation time (43.8 ± 15.8 minutes vs 51.6 ± 18.7 minutes; P < 0.001) and lower estimated blood loss (EBL, 6.5 ± 7.8 mL vs 8.6 ± 8.3 mL; P < 0.001) than MPLA. No significant differences were observed in complications, pain scores, or length of hospital stay. SPLA was not inferior to MPLA in the main outcomes, except for the complication rate, where statistical power was insufficient. Multivariable regression confirmed SPLA as an independent factor for operation time and EBL.
Conclusion: SPLA is more feasible than MPLA for retrocecal appendicitis, offering advantages in operation time and estimated blood loss. This study supports SPLA as a viable alternative that enhances postoperative recovery.
Keywords: Laparoscopic appendectomy; Multi-port laparoscopic appendectomy; Propensity score matching; Retrocecal appendicitis; Single-port laparoscopic appendectomy.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that there are no conflicts of interest.
Figures
References
-
- Han Y, Yuan H, Li S, Wang WF. Single-incision versus conventional three-port laparoscopic appendectomy for acute appendicitis: A meta-analysis of randomized controlled trials. Asian J Surg. 2024;47:864–873. - PubMed
-
- Cirocchi R, Cianci MC, Amato L, Properzi L, Buononato M, Di Rienzo VM, Tebala GD, Avenia S, Iandoli R, Santoro A, Vettoretto N, Coletta R, Morabito A. Laparoscopic appendectomy with single port vs conventional access: systematic review and meta-analysis of randomized clinical trials. Surg Endosc. 2024;38:1667–1684. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
