

Intra-abdominal sepsis in critically ill surgical patients: the relationship between cumulative fluid balance and serum sodium and chloride levels and in-hospital mortality
- PMID: 40740943
- PMCID: PMC12307356
- DOI: 10.3389/fmed.2025.1608388
Intra-abdominal sepsis in critically ill surgical patients: the relationship between cumulative fluid balance and serum sodium and chloride levels and in-hospital mortality
Abstract
Background and aim: Intra-abdominal sepsis in critically ill surgical patients has a high mortality rate. Fluid therapy is essential resuscitation measure but can lead to poor outcome due to fluid overload and increased sodium and chloride levels. This study aimed to examine the relationship between cumulative fluid balance, serum sodium and chloride levels in the intensive care unit (ICU), and in-hospital mortality in critically ill surgical patients with intra-abdominal sepsis.
Methods: The study was designed as a retrospective, observational study. Data were collected and analyzed from 100 critically ill surgical patients with intra-abdominal sepsis who were immediately subjected to surgical treatment. Postoperative care continued in the ICU for at least 7 days. Data related to daily fluid enteral and parenteral intake and loss were taken from medical records. The cumulative fluid balance was calculated for the periods from days 1 to 3 and 1 to 7 of ICU treatment.
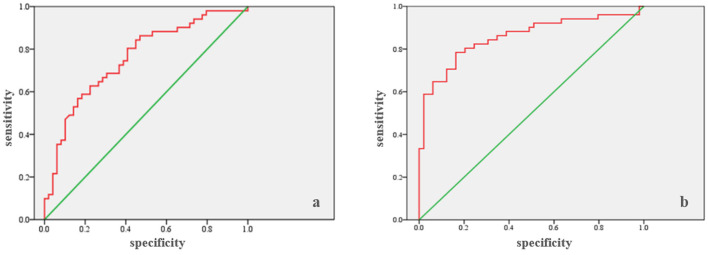
Results: In-hospital mortality rate was 51%. The cumulative fluid balance on the third and seventh days of ICU hospitalization was found to be positively correlated with mortality. Statistical analyses revealed significant differences in fluid balance at these time points in relation to mortality (p < 0.0005). ROC analysis confirmed the predictive power of cumulative fluid balance, with an AUC of 0.757 (cutoff: 5,130 ml, sensitivity 68.6%, specificity 69.4%) on the third day and AUC of 0.856 (cutoff: 2,210 ml, sensitivity 78.4%, specificity 83.7%) on the seventh day. Binary logistic regression further supported the influence of fluid balance on mortality. Sodium and chloride levels remained within the reference range but were significantly higher in patients who died. Binary logistic regression showed that abnormal sodium and chloride levels on the third and seventh days were associated with increased mortality.
Conclusion: High values of postoperative cumulative fluid balance as well as elevated serum sodium and chloride levels during the first 7 days in the ICU may be important predictors of in-hospital mortality in critically ill patients with intra-abdominal sepsis who underwent emergency surgical treatment.
Clinical trial registration: https://clinicaltrials.gov/study/NCT06838585?locStr=Novi%20Sad,%20Serbia&country$=$Serbia&state$=$Vojvodina&city$=$Novi%20Sad&cond$=$intra%20abdominal%20sepsis&rank$=$3, NCT06838585.
Keywords: chlorides; fluid balance; fluid therapy; in-hospital mortality; intra-abdominal sepsis; sodium.
Copyright © 2025 Popović, Anđelić, Jovanović, Maričić Prijić, Uvelin, Tomić, Plećaš Ðurić, Todorović, Milijašević and Marković.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- World Health Organization . Sepsis. Geneva: WHO; (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/sepsis [Accessed March 20, 2025].
Associated data
LinkOut - more resources
Full Text Sources
Medical