

Association of Neutrophil Percentage-to-Albumin Ratio with All-Cause and Cardiovascular Mortality in Maintenance Hemodialysis Patients: A Retrospective Study
- PMID: 40740971
- PMCID: PMC12309577
- DOI: 10.2147/JIR.S532319
Association of Neutrophil Percentage-to-Albumin Ratio with All-Cause and Cardiovascular Mortality in Maintenance Hemodialysis Patients: A Retrospective Study
Abstract
Aim: Patients undergoing maintenance hemodialysis (MHD) are prone to chronic inflammation, which often leads to the elevation of various inflammatory biomarkers. This study aims to investigate whether the neutrophil percentage-to-albumin ratio (NPAR), a novel biomarker linked to inflammation, increases the likelihood of both overall and cardiovascular mortality in these patients.
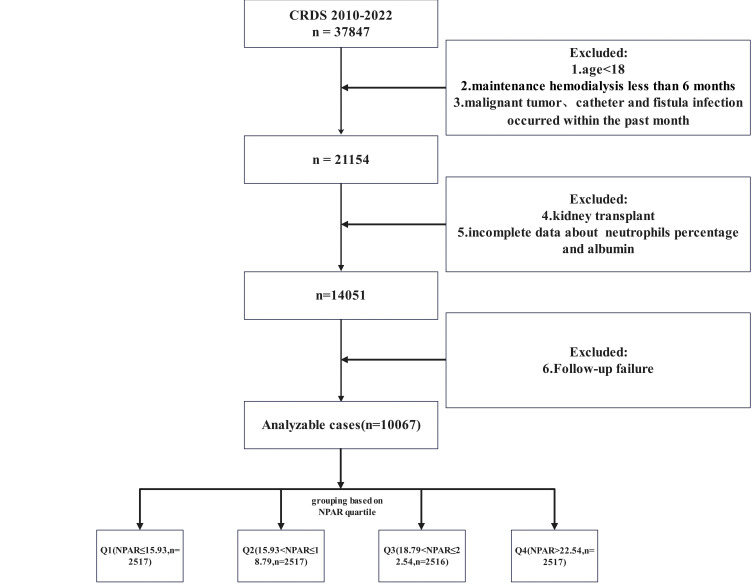
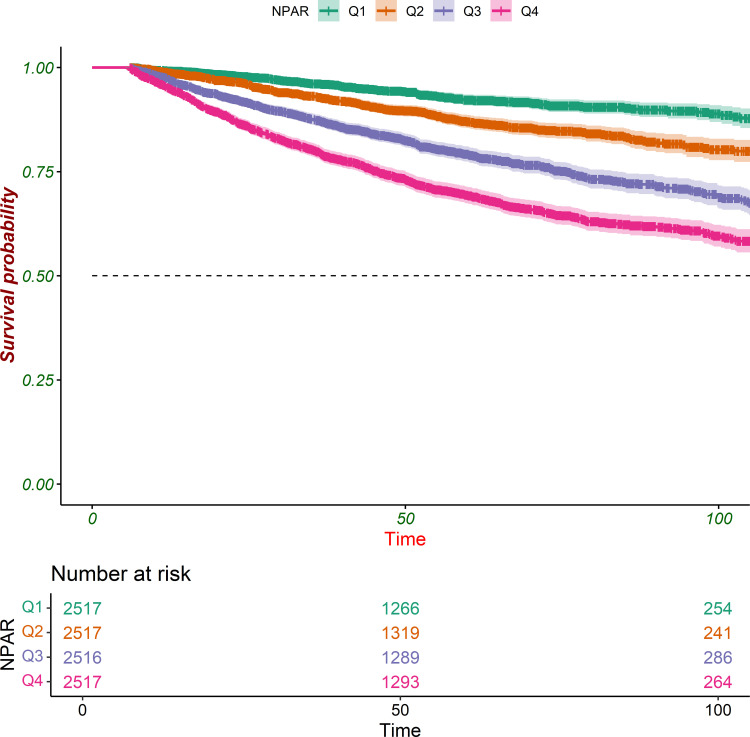
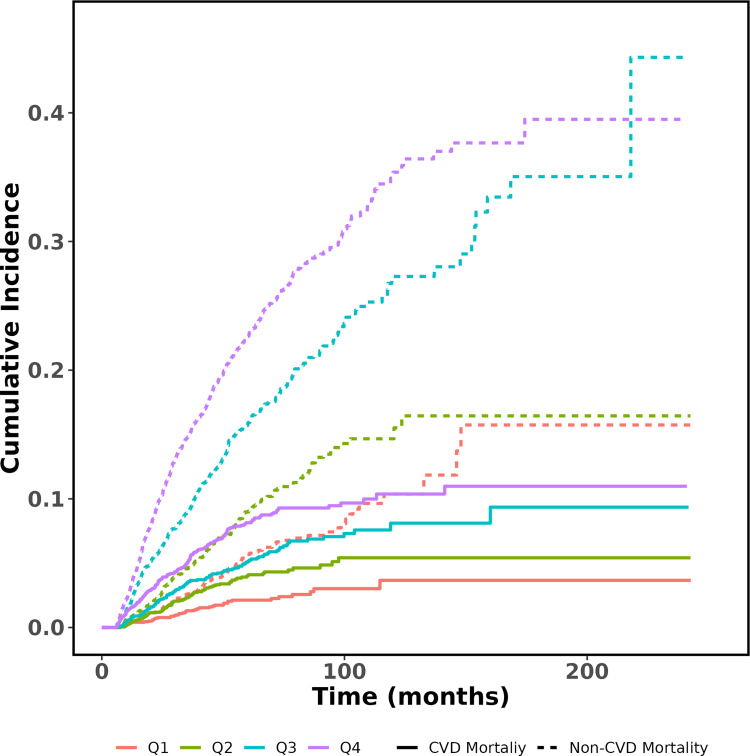
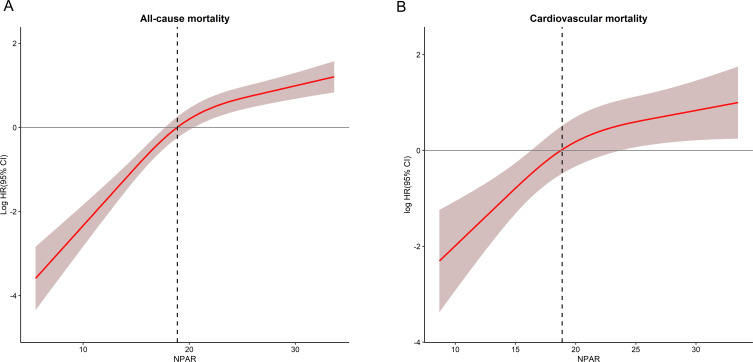
Methods: This retrospective cohort study, conducted across multiple centers, utilized data from the China Renal Data System (CRDS) Database collected between 2010 and 2022. A total of 10,067 eligible participants were included, with follow-up data available until December 31, 2022. Univariate and multivariate Cox regression analyses, Kaplan-Meier survival curves, competing risk plots, and restricted cubic splines were applied to investigate the association between NPAR and both overall and cardiovascular mortality in patients undergoing MHD. Additionally, time-dependent ROC analysis and C-index were employed to assess the predictive ability of NPAR for short-term and long-term outcomes in MHD patients.
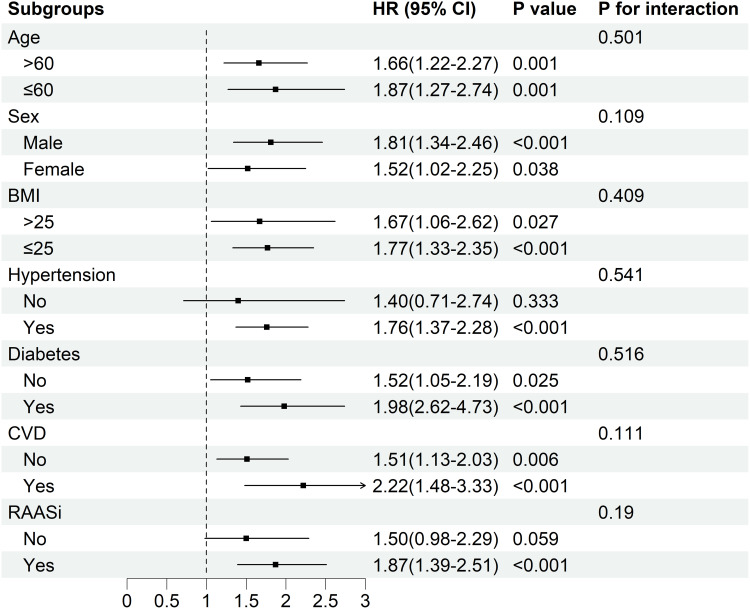
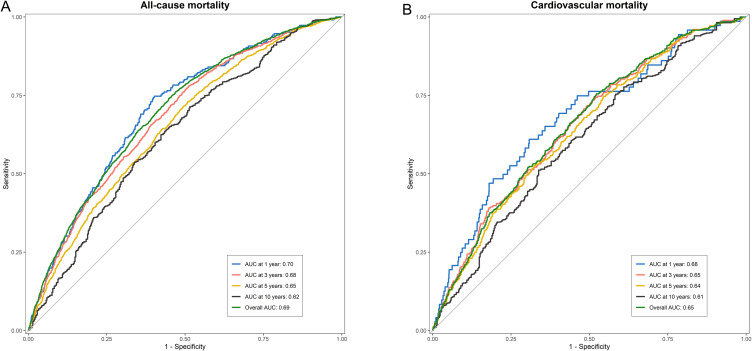
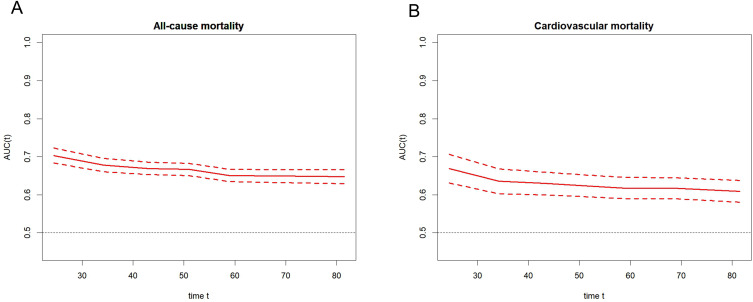
Results: Among 10,067 eligible individuals, 1759 deaths from any cause were recorded over a median follow-up period of 50.9 months, with 453 of these deaths attributed to cardiovascular causes. Multivariate Cox regression models revealed that high NPAR levels were significantly associated with both all-cause mortality (HR 3.73, 95% CI 2.94-4.73) and cardiovascular mortality (HR 2.38, 95% CI 1.50-3.79). In subgroup analysis, the effect of elevated NPAR levels on the prediction of all-cause mortality was consistent across the seven pre-specified subgroup strata (all P for interaction > 0.05). Sensitivity analysis confirmed that NPAR remained significantly associated with all-cause mortality. Time-dependent ROC analysis showed that the AUC for NPAR in predicting all-cause mortality at overall, 1, 3, 5, and 10 years was 0.69, 0.70, 0.68, 0.65, and 0.62, respectively. For cardiovascular mortality, the corresponding values were 0.65, 0.68, 0.65, 0.64, and 0.61, respectively. For all-cause mortality, the adjusted C-index was 0.76 (95% CI: 0.74-0.78), while for cardiovascular mortality, the adjusted C-index was 0.82 (95% CI: 0.79-0.85).
Conclusion: In MHD patients, elevated NPAR levels were significantly associated with an increased risk of both overall and cardiovascular mortality, and demonstrated greater accuracy in predicting short-term outcomes.
Keywords: China renal data system database; all-cause mortality; cardiovascular mortality; hemodialysis; neutrophil percentage-to-albumin ratio.
© 2025 Jiang et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
