

Practical Applications of Lung and Diaphragm Ultrasound in the Intensive Care Unit: An Updated Narrative Review
- PMID: 40741034
- PMCID: PMC12309786
- DOI: 10.7759/cureus.88584
Practical Applications of Lung and Diaphragm Ultrasound in the Intensive Care Unit: An Updated Narrative Review
Abstract
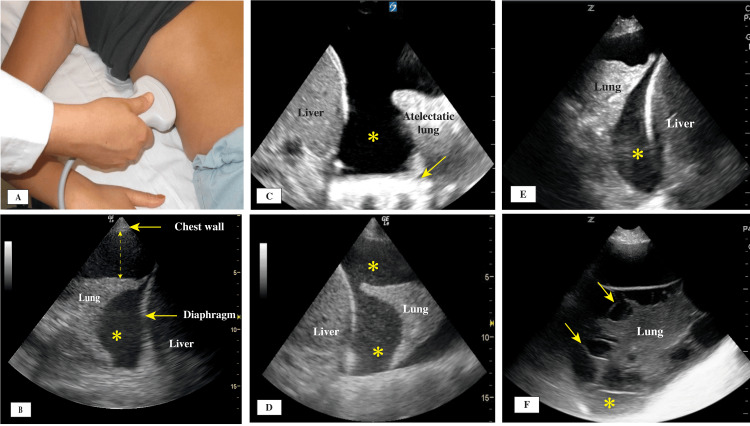
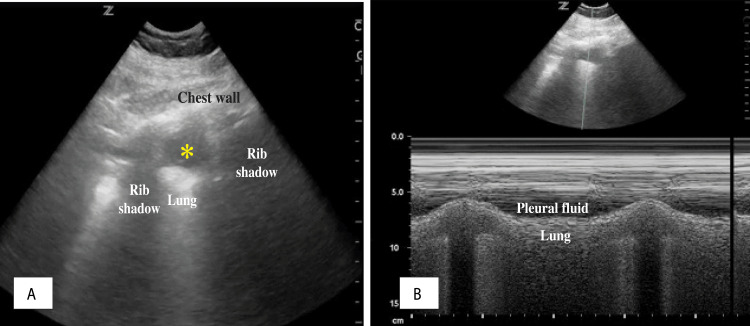
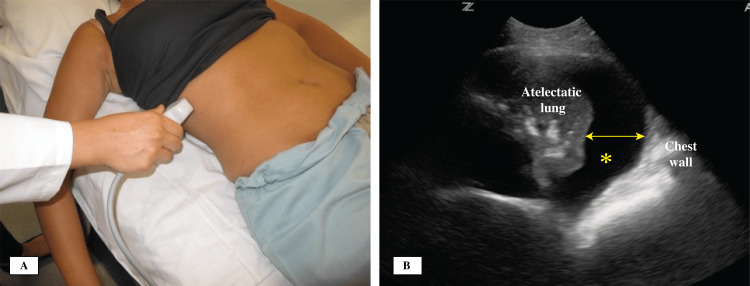
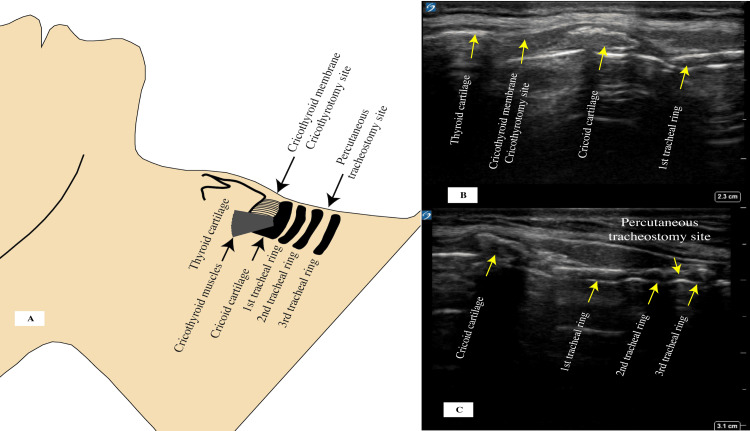
Lung ultrasound (LUS) has evolved significantly during the past few decades. Its use has been integrated into daily practices of intensive care units (ICUs) worldwide, and it has proven to be a valuable tool in the assessment and management of patients with respiratory failure caused by lung, pleural, diaphragmatic, and other diseases. LUS techniques are becoming increasingly standardized, which can help in interpreting data and improving patients' outcomes. In this narrative review, the focus was on the practical daily applications of lung, pleural, and diaphragmatic ultrasound with emphasis on different signs and artifacts that guide the interpretation of data and identification of disease. Discussions and analysis from the new international guidelines were added to help close the gap in the use of LUS. This review is intended to serve as a practical guide for using bedside ultrasound in evaluating patients with shortness of breath and respiratory failure and to provide guidance to help providers manage patients and generate standardized reports. We start with an analysis of best practices and guidelines on performing an LUS exam in the ICU setting. This analysis is followed by data interpretation of findings starting at the pleural line and traveling deeper into the lung tissue. The review includes discussions of the diaphragm evaluation and its function and abnormalities, as well as common LUS-related procedures in the ICU, such as thoracentesis, tracheostomy, and cricothyrotomy.
Keywords: a-lines; acute respiratory distress syndrome (ards); b-lines; diaphragm ultrasound (d-usg); lung ultrasound (lus); percutaneous tracheostomy; pleural fluid (pf); pleural ultrasound; pneumonia; point-of-care ultrasound (pocus).
Copyright © 2025, Killu et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Ultrasound for routine clinical investigations. Pell RL. Ultrasonics. 1964;2:87–89.
-
- International evidence-based recommendations for point-of-care lung ultrasound. Volpicelli G, Elbarbary M, Blaivas M, et al. Intensive Care Med. 2012;38:577–591. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous