

Clinical efficacy of surgically assisted transjugular intrahepatic portosystemic shunt for cavernous transformation of portal vein
- PMID: 40741105
- PMCID: PMC12305199
- DOI: 10.3748/wjg.v31.i27.108483
Clinical efficacy of surgically assisted transjugular intrahepatic portosystemic shunt for cavernous transformation of portal vein
Abstract
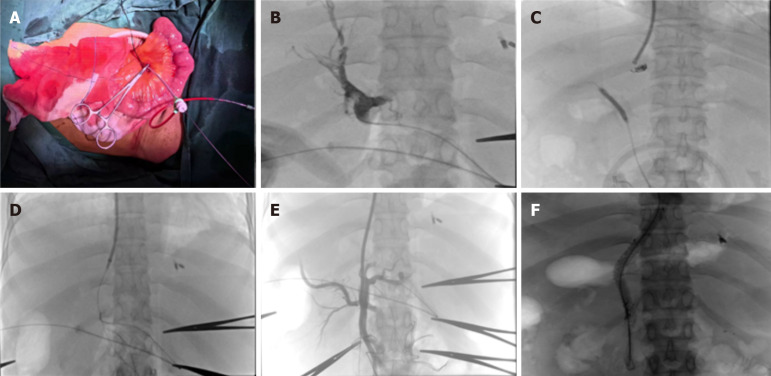
Background: Transjugular intrahepatic portosystemic shunt (TIPS) is contraindicated for patients with cavernous transformation of the portal vein (CTPV) due to high surgery-related mortality risk. However, surgically assisted TIPS (SATIPS) can significantly reduce the risk.
Aim: To evaluate the clinical efficacy of SATIPS, this study was conducted.
Methods: One hundred and seven patients with CTPV and esophagogastric variceal bleeding were recruited from January 2023 to December 2024.The patients were recruited from three different hospitals. Overall, 54 patients received SATIPS treatment (SATIPS group), while 53 patients did not receive SATIPS and underwent prophylactic endoscopic sclerosing ligation (control group). Subsequently, survival rates, incidence rates of gastrointestinal bleeding, incidence of hepatic encephalopathy rate, and the incidence of liver failure after treatment in both groups at 3 and 6 months were observed.
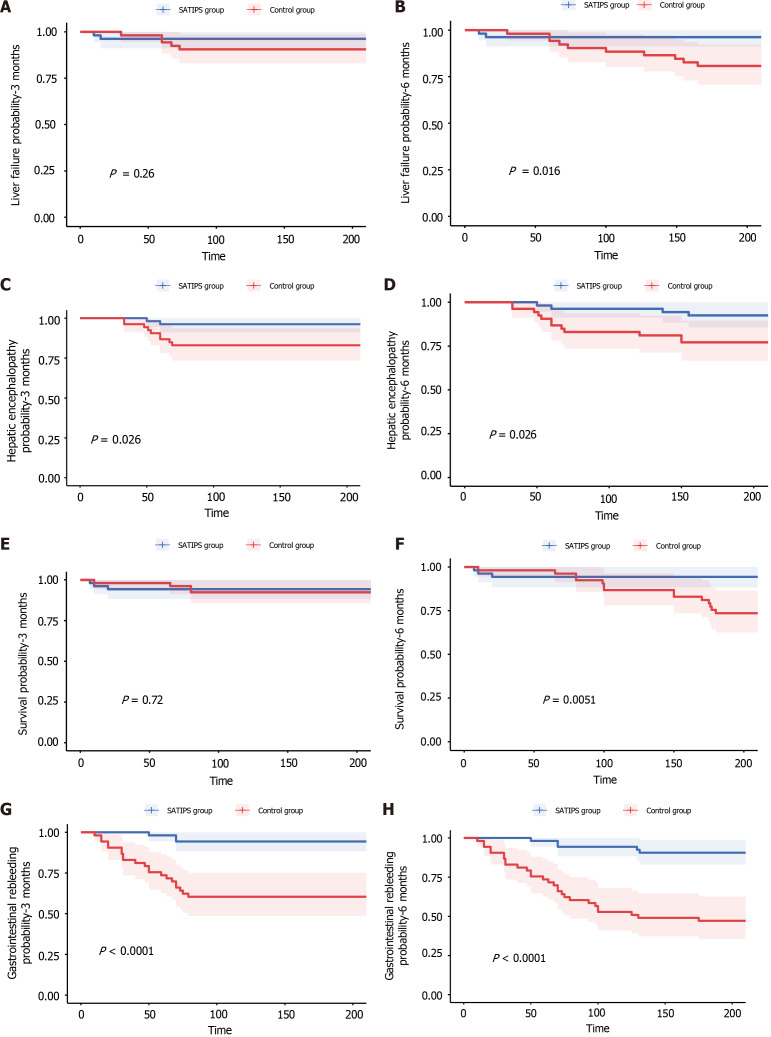
Results: The survival rates for the SATIPS and control groups were 94.4% and 92.5% at 3 months (P value = 0.72) and 94.4% and 73.6% at 6 months (P value = 0.0051) respectively. The incidence of liver failure was 3.7% and 9.4% at 3 months (P value = 0.26) and 3.7% and18.9% at 6 months (P value = 0.016); the incidence of gastrointestinal bleeding was 5.6% and 37.7% at 3 months (P value < 0.001) and 9.3% and 47.2% (P value < 0.001) at 6 months; and the incidence of hepatic encephalopathy was 3.7% and 17.0% at 3 months (P value = 0.026) and 7.4% and 26.4% at 6 months (P value = 0.026) respectively.
Conclusion: For patients with CTPV, there were no optimal treatment. Regarding long-term efficacy, SATIPS can significantly reduce the rate of rebleeding, hepatic encephalopathy and liver failure, and is associated with better survival.
Keywords: Cavernous transformation of portal vein; Esophagogastric variceal bleeding; Portal hypertension; Portal vein thrombosis; Surgically assisted transjugular intrahepatic portosystemic shunt.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
Similar articles
-
Identifying the optimal measurement timing and hemodynamic targets of portal pressure gradient after TIPS in patients with cirrhosis and variceal bleeding.J Hepatol. 2025 Feb;82(2):245-257. doi: 10.1016/j.jhep.2024.08.007. Epub 2024 Aug 22. J Hepatol. 2025. PMID: 39181214
-
Transjugular Splenocaval Shunt Creation for the Treatment of Portal Vein Cavernous Transformation with Recurrent Variceal Hemorrhage.J Vasc Interv Radiol. 2025 Aug;36(8):1330-1335. doi: 10.1016/j.jvir.2025.05.002. Epub 2025 May 11. J Vasc Interv Radiol. 2025. PMID: 40360012
-
Transjugular intrahepatic portosystemic shunt prevents rebleeding in cirrhotic patients having cavernous transformation of the portal vein without improving their survival.J Dig Dis. 2019 Feb;20(2):89-96. doi: 10.1111/1751-2980.12702. Epub 2019 Mar 3. J Dig Dis. 2019. PMID: 30629804
-
Secondary prevention of variceal bleeding in adults with previous oesophageal variceal bleeding due to decompensated liver cirrhosis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Mar 30;3(3):CD013122. doi: 10.1002/14651858.CD013122.pub2. Cochrane Database Syst Rev. 2021. PMID: 33784794 Free PMC article.
-
Endoscopic injection of cyanoacrylate glue versus other endoscopic procedures for acute bleeding gastric varices in people with portal hypertension.Cochrane Database Syst Rev. 2015 May 12;2015(5):CD010180. doi: 10.1002/14651858.CD010180.pub2. Cochrane Database Syst Rev. 2015. PMID: 25966446 Free PMC article.
References
-
- Bloom S, Kemp W, Lubel J. Portal hypertension: pathophysiology, diagnosis and management. Intern Med J. 2015;45:16–26. - PubMed
-
- Buob S, Johnston AN, Webster CR. Portal hypertension: pathophysiology, diagnosis, and treatment. J Vet Intern Med. 2011;25:169–186. - PubMed
-
- Rozenblit G, Del Guercio LR. Combined transmesenteric and transjugular approach for intrahepatic portosystemic shunt placement. J Vasc Interv Radiol. 1993;4:661–666. - PubMed
-
- Jalaeian H, Talaie R, D'Souza D, Taleb S, Noorbaloochi S, Flanagan S, Hunter D, Golzarian J. Minilaparotomy-Assisted Transmesenteric-Transjugular Intrahepatic Portosystemic Shunt: Comparison with Conventional Transjugular Approach. Cardiovasc Intervent Radiol. 2016;39:1413–1419. - PubMed
-
- Wang L, Peng Y, Qian Y, Liu Z, Du J, Meng Y, Feng L, Dai Z, Xu L. Transjugular extrahepatic portosystemic shunt (TEPS) creation in patients with complete occlusion of portal vein: Primary experience in a single medical center. Clin Res Hepatol Gastroenterol. 2022;46:101786. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
