

Elevated stress hyperglycemia ratio associated with higher hospital mortality in patients with respiratory failure
- PMID: 40744965
- PMCID: PMC12314029
- DOI: 10.1038/s41598-025-12853-3
Elevated stress hyperglycemia ratio associated with higher hospital mortality in patients with respiratory failure
Abstract
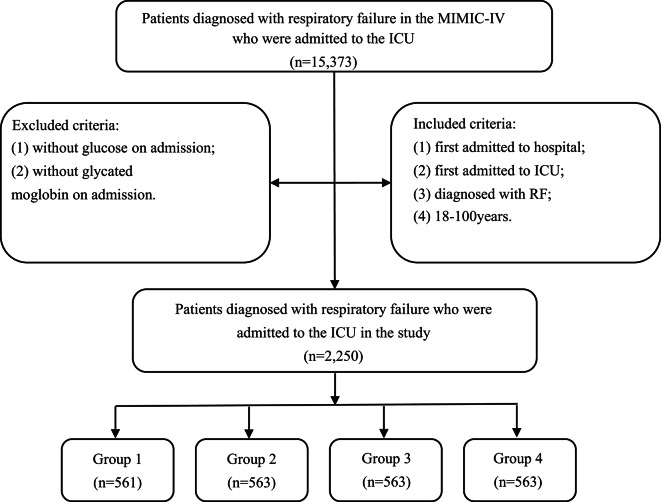
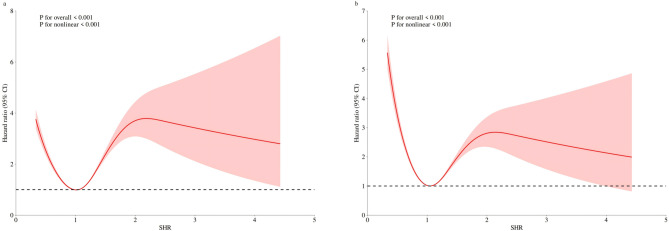
The stress hyperglycemia ratio (SHR) represents an emerging biomarker linked to poor clinical outcomes. However, its association with fatal outcomes in patients experiencing respiratory failure (RF) remains poorly understood. This research was designed to evaluate the utility of SHR in predicting both in-hospital mortality and intensive care unit (ICU) mortality among RF patients. This retrospective cohort analysis utilized data from the MIMIC-IV version 3.0 database. Patients diagnosed with RF in the ICU were divided into four groups according to the SHR index quartiles (group1, group2, group3, and group4), and the outcomes were in-hospital and ICU mortality. Survival outcomes among different groups were analyzed through Kaplan-Meier curves. Based on the results of the schoenfeld residual test, choose the Cox model or the model with the time interaction term to report the association between SHR and the outcome. Furthermore, restricted cubic splines analyses were conducted to explore potential non-linear relationships of SHR with both in-hospital and ICU mortality. This study enrolled 2,250 participants, demonstrating in-hospital mortality and ICU mortality rates of 23.91% and 14.31%, respectively. Kaplan-Meier analysis revealed that the group4 exhibited the lowest survival rates (P < 0.001). Through multivariate Cox regression, when comparing the group1 to the group4, three analytical models consistently showed increased in-hospital and ICU mortality in group4. The time interaction model revealed significant increases in hospital mortality risk across SHR quartiles compared to group1. Specifically, in model1, group2 showed a 62%-69% higher risk (HR = 1.69, 95% CI: 1.17-2.44), group3 exhibited a 358%-370% higher risk (HR = 4.58, 95% CI: 1.83-11.5) ,while group4 demonstrated exponential risk escalation. All quartile groups exhibited a daily risk attenuation of approximately 57% (time interaction term HR = 0.43, all p < 0.001). The associations remained consistent after adjusting the variables in models 2 and 3. In contrast, no significant risk association was observed between SHR and ICU mortality in the time interaction model. Besides, a U-shaped relationship was observed between SHR and both in-hospital mortality and ICU mortality. The study revealed that elevated SHR levels in ICU-admitted RF patients were significantly associated with increased risks of in-hospital mortality. Clinicians should closely monitor patients with high admission SHR values, especially patients in the highest SHR quantile (Q4 group) during the early admission period, underscoring the need for prioritized clinical intervention in this high-risk population.
Keywords: ICU mortality; In-hospital mortality; Intensive care unit; MIMIC-IV; Respiratory failure; Stress hyperglycemia ratio.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: This study was conducted according to the guidelines of the Declaration of Helsinki. The review boards of the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center approved the use of the MIMIC-IV database. Because the data were publicly available, the study was exempt from the requirements of an ethics approval statement and informed consent.
Figures



Similar articles
-
Stress hyperglycemia ratio as a biomarker for early mortality risk stratification in cardiovascular disease: a propensity-matched analysis.Cardiovasc Diabetol. 2025 Jul 12;24(1):286. doi: 10.1186/s12933-025-02812-7. Cardiovasc Diabetol. 2025. PMID: 40652236 Free PMC article.
-
Association of stress hyperglycemia ratio with mortality in sepsis-associated acute kidney injury: a retrospective analysis of the MIMIC-IV database.Sci Rep. 2025 Aug 20;15(1):30667. doi: 10.1038/s41598-025-16783-y. Sci Rep. 2025. PMID: 40835690 Free PMC article.
-
Correlation between stress hyperglycemic ratio and all-cause mortality in diabetic patients with heart failure.BMC Endocr Disord. 2025 Aug 6;25(1):192. doi: 10.1186/s12902-025-02010-2. BMC Endocr Disord. 2025. PMID: 40770315 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
High-flow nasal cannulae for respiratory support in adult intensive care patients.Cochrane Database Syst Rev. 2017 May 30;5(5):CD010172. doi: 10.1002/14651858.CD010172.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2021 Mar 4;3:CD010172. doi: 10.1002/14651858.CD010172.pub3. PMID: 28555461 Free PMC article. Updated.
References
-
- Vincent, J. L. et al. The epidemiology of acute respiratory failure in critically ill patients(*). Chest121, 1602–1609 (2002). - PubMed
-
- Chen, L. & Rackley, C. R. Diagnosis and epidemiology of acute respiratory failure. Crit. Care Clin.40, 221–233 (2024). - PubMed
-
- Ippolito, M., Galvano, A. N. & Cortegiani, A. Long-term outcomes in critically ill patients with acute respiratory failure. Curr. Opin. Crit. Care. 30, 510–522 (2024). - PubMed
-
- Bellani, G. et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. Jama-J Am. Med. Assoc.315, 788–800 (2016). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
