

A pilot study on the hemodynamic effects of negative pressure ventilation in patients after cardiac surgery focussing on right ventricular function
- PMID: 40744972
- PMCID: PMC12314026
- DOI: 10.1038/s41598-025-12534-1
A pilot study on the hemodynamic effects of negative pressure ventilation in patients after cardiac surgery focussing on right ventricular function
Abstract
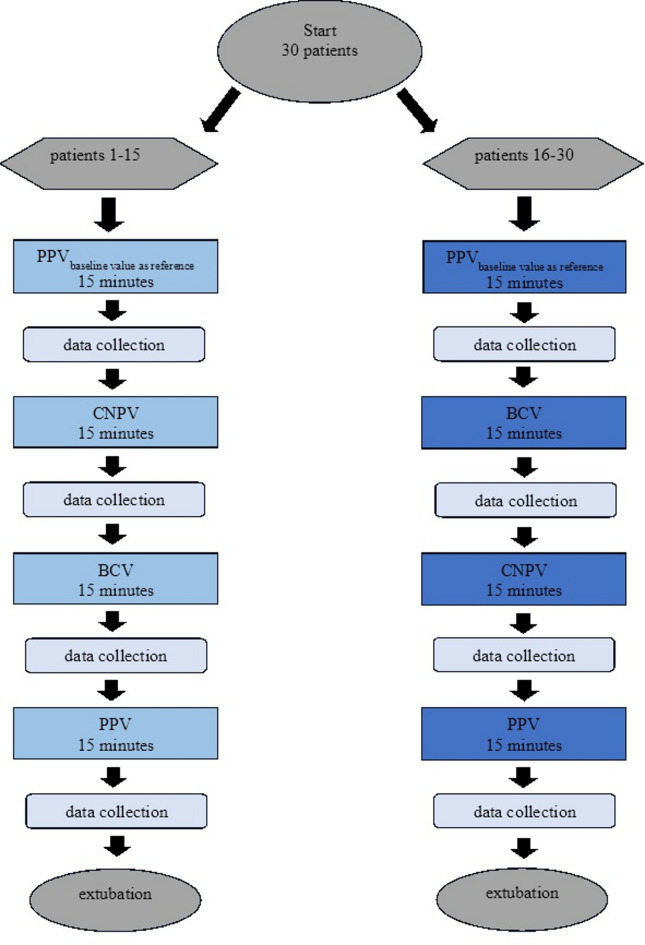
Right ventricular dysfunction and right ventricular failure are important complications in cardiac surgical patients and typically observed after complex surgical cases. Treatment options for optimizing the hemodynamic status in patients presenting with these complications are limited. Negative pressure ventilation has been shown to ameliorate the effects of conventional positive pressure ventilation (PPV) and to improve cardiac output in patients with Fontan circulation and patients undergoing coronary artery bypass surgery. No data are available on the effects of negative pressure ventilation on systemic hemodynamics and right heart function after complex on-pump cardiac surgery. Hypothesis of the present study is that right ventricular function improves under condition of negative pressure ventilation after complex on-pump surgery. Thirty patients after complex cardiac surgery were examined using basic hemodynamic monitoring, transesophageal ultrasound, a 3rd generation pulmonary artery catheter, cerebral oximetry and arterial and venous blood gases. The first 15 patients were ventilated for 15 min using standard PPV followed by 15 min of extrathoracal continuous negative pressure ventilation (CNPV) combined with PPV, and 15 min of extrathoracal biphasic negative pressure ventilation (BCV, biphasic cuirass ventilation) combined with an as far as possible reduced PPV. In the second 15 patients, the sequence of negative pressure ventilation was changed and BCV was performed before CNPV. Finally, every patient was ventilated for 15 min with standard PPV again. A full dataset of hemodynamics and a respiratory dataset was collected during each observation period. CNPV und BCV reduced central venous pressure and pulmonary artery occlusion pressure by 2 mmHg. During BCV cardiac index increased by + 24% (+ 0.5 l/min/m2; 95% CI 0.2-0.8, p = 0.001) through an increase of stroke volume index by + 24% (p = 0.0003) without change of heart rate. This was accompanied by an increase of right ventricular ejection fraction (+ 18%, p = 0.008), pulmonary arterial pulsatility index (+ 30%, p = 0.0001), left ventricular ejection fraction (+ 15%, p = 0.01), and oxygen delivery DO2 (+ 13%, p = 0.0006). Posthoc analysis in patients with reduced stroke volume index (< 27 ml/m2 prior to the start of the study) revealed that mixed venous oxygen saturation and cerebral oxygen saturation increased by 7% (p = 0.005/p = 0.006). No adverse effects were observed. While CNPV has only moderate hemodynamic effects by reducing cardiac filling pressure, BCV improves systemic and right ventricular hemodynamics as well as global oxygen balance in patients after complex cardiac surgery. During both negative pressure ventilation modes, no immediate adverse events could be observed. These findings justify investigations if these treatment modalities may impact clinical outcomes in patients with right ventricular dysfunction or failure.Trial registration clinicaltrials.gov ID: NCT06088966, registered October 3rd, 2023.
Keywords: Cardiac surgery; Heart failure; Hemodynamic optimization; Negative pressure ventilation; Right ventricular failure.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: The study was approved by the local ethics committee (reference number BB 041/23, Ethikkommission der Universität Greifswald, Felix-Hausdorff-Straße 3, 17487 Greifswald). Written consent of every patient was obtained before considering inclusion.
Figures


Similar articles
-
Ventilator Management(Archived).2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 28846232 Free Books & Documents.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Positioning for acute respiratory distress in hospitalised infants and children.Cochrane Database Syst Rev. 2022 Jun 6;6(6):CD003645. doi: 10.1002/14651858.CD003645.pub4. Cochrane Database Syst Rev. 2022. PMID: 35661343 Free PMC article.
-
Hemodynamic Effects of Altering Tidal Volume During Positive Pressure Ventilation in the Fontan Circulation: A Randomized Crossover Trial.Paediatr Anaesth. 2025 Aug;35(8):607-618. doi: 10.1111/pan.15096. Epub 2025 Mar 19. Paediatr Anaesth. 2025. PMID: 40105302 Clinical Trial.
-
Music interventions for mechanically ventilated patients.Cochrane Database Syst Rev. 2014;2014(12):CD006902. doi: 10.1002/14651858.CD006902.pub3. Epub 2014 Dec 9. Cochrane Database Syst Rev. 2014. PMID: 25490233 Free PMC article.
References
-
- Haddad, F. et al. The right ventricle in cardiac surgery, a perioperative perspective: II. Pathophysiology, clinical importance, and management. Anesth. Analg.108(2), 422–433. 10.1213/ane.0b013e31818d8b92 (2009). - PubMed
-
- Alnsasra, H. et al. Pericardiocentesis induced right ventricular changes in patients with and without pulmonary hypertension. Echocardiography38(5), 752–759. 10.1111/echo.15046 (2021). - PubMed
-
- Singh, A. et al. Right ventricular function is reduced during cardiac surgery independent of procedural characteristics, reoperative status, or pericardiotomy. J. Thorac. Cardiovasc. Surg.159(4), 1430–1438. 10.1016/j.jtcvs.2019.04.035 (2020). - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
