

Distress screening in patients with high-grade glioma: diagnostic accuracy in relation to a structured clinical interview in a multicenter cluster-randomized controlled trial
- PMID: 40745114
- PMCID: PMC12313720
- DOI: 10.1007/s00520-025-09810-1
Distress screening in patients with high-grade glioma: diagnostic accuracy in relation to a structured clinical interview in a multicenter cluster-randomized controlled trial
Abstract
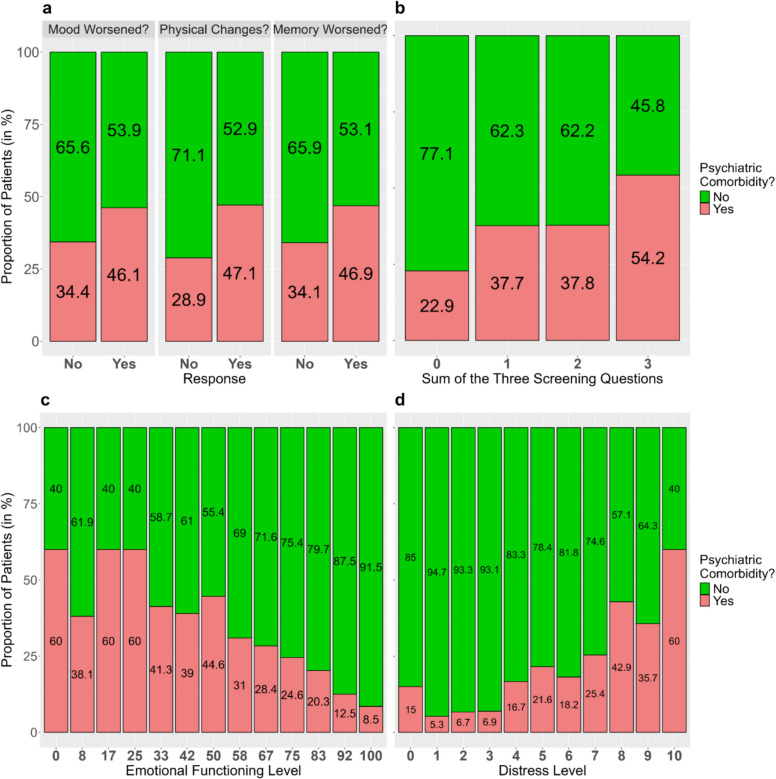
Purpose: Structured clinical interviews, such as the Structured Clinical Interview for DSM (SCID), are considered the gold standard for diagnosing mental disorders but are challenging in routine clinical use due to their length. Therefore, screening instruments to identify the need for further assessment are required. The National Comprehensive Cancer Network Distress Thermometer (DT) screens for psychological distress, while the Emotional Functioning (EF) scale of the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core (EORTC QLQ-C30) assesses emotional functioning. Both are frequently used in clinical routine. Additionally, three brief screening questions (TSQ), specifically developed for patients with glioma and integrated into doctor-patient consultations, may also be used for screening. This study aimed to evaluate the ability of the three tools to identify patients with psychiatric comorbidities as diagnosed by the SCID.
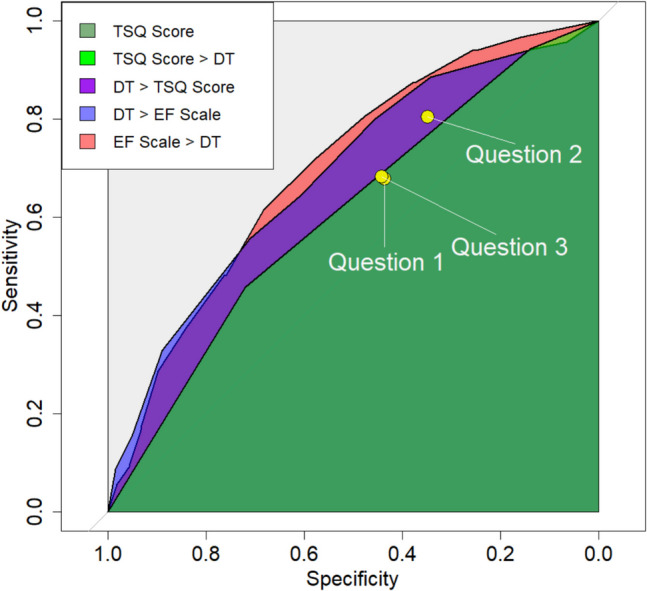
Methods: Using data from glioma patients treated at 13 German hospitals participating in a cluster-randomized trial, discriminative abilities were assessed using receiver operating characteristic (ROC) curves and corresponding areas under the curve (AUCs). Confidence intervals (CIs) were estimated, and hypothesis tests were conducted using bootstrapping.
Results: Of the 691 patients interviewed, 31% presented with at least one mental disorder. The EF scale demonstrated the best discriminative ability (AUC 0.70, 95% CI: 0.66-0.74), followed by the DT (AUC 0.69, 95% CI: 0.62-0.76), and the TSQ total score (AUC 0.61, 95% CI: 0.55-0.66).
Conclusion: While all three tools performed better than random chance, none demonstrated convincing discriminative ability in identifying psychiatric comorbidities. In practice, screening tools can identify a substantial proportion of patients with mental disorders, however at the cost of a considerable number of false negatives.
Keywords: Emotional distress; High-grade glioma; Mental disorder; Psychological burden; Screening tool; Structured clinical interview (SCID).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: Susanne Singer reports honoraria from Lilly Deutschland; outside the submitted work. Joachim Steinbach has received honoraria for presentations, educational events and advisory board participation from GSK, Boehringer Ingelheim, Roche, Novocure, Seagen, Servier and Med-Update. Martin Misch reports travel support and support for other professional activities from Novocure outside the submitted work. Mirjam Renovanz reports grants/contracts from Novocure outside the submitted work. The remaining authors disclosed no conflicts of interest. Ethical approval: Ethical approval for this study was obtained from the Ethics Review Board of the Medical Association of Rhineland-Palatinate (reference number: 837.170–17[11013]). The research was conducted in accordance with the principles outlined in the guidelines of the Declaration of Helsinki and the International Council for Harmonisation – Good Clinical Practice (ICH-GCP). Consent to participate: Written informed consent was obtained from all participants prior to their inclusion in the study.
Figures
References
Publication types
MeSH terms
Grants and funding
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
- 01VSF18011/Federal Joint Committee (Gemeinsamer Bundesausschuss)
LinkOut - more resources
Full Text Sources
Medical
