

A comparison of deep versus awake tracheal extubation in adults: a randomized controlled trial
- PMID: 40745279
- PMCID: PMC12315347
- DOI: 10.1186/s12871-025-03224-6
A comparison of deep versus awake tracheal extubation in adults: a randomized controlled trial
Abstract
Background: Awake extubation is deemed a generally safe option for tracheal extubation in low-risk patients, while anesthetized, or"deep" extubation is often considered best suited to seasoned providers due to its perceived hazards. However, inadequate data exists about the relative safety of deep and awake extubations in the adult population.
Methods: Adult patients (n=220) with favorable airways undergoing elective surgeries under general tracheal anesthesia were enrolled prospectively. Following a standardized volatile anesthetic regimen, patients were randomized to undergo deep or awake tracheal extubation. The primary outcome was the occurrence of at least one airway or respiratory complication. Secondary outcomes included airway interventions, hemodynamic parameters, severe emergence agitation, and sore throat severity.
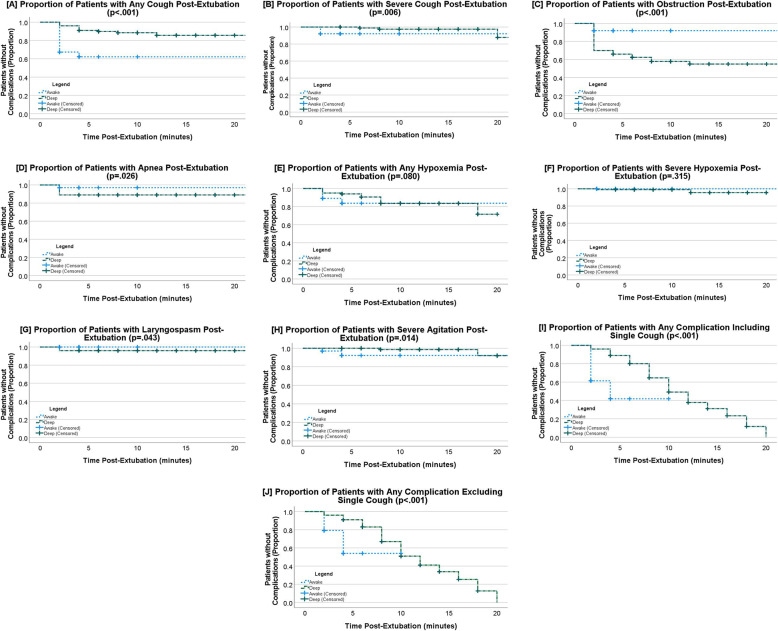
Results: Pre-extubation, awake extubations exhibited an increased rate of any airway and respiratory complications (risk ratio [RR] - 5.1; 95% confidence interval [CI] - 2.8-9.5; p<.001), attributable to greater incidences of cough (RR - 6.8; 95% CI - 3.2-14.3, p>.001) and hypoxemia (RR - 3.6; 95% CI - 1.3-10.6, p=.010). After extubation, a significantly decreased rate of one or more complications occurred in the awake extubation group (RR - 0.7; 95% CI - 0.6-1.0; p=.028). Awake extubations were associated with fewer incidences of airway obstruction (RR - 0.2; 95% CI - 0.1-0.4, p<.001) and apnea (RR - 0.3; 95% CI - 0.1-0.9; p=.025), but higher rates of any severity cough (RR - 2.9; 95% CI - 1.6-5.2; p<.001). Awake extubations required significantly fewer airway interventions after extubation (RR - 0.2; 95% CI - 0.1-0.6; p<.001). No serious adverse events occurred.
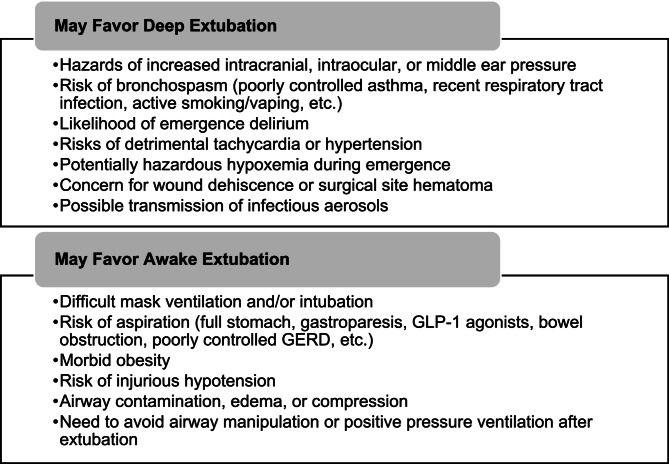
Conclusions: Deep and awake extubations produce distinct airway and respiratory complication profiles, without either being conclusively safer. The risks posed by each technique during emergence and after extubation should be considered by anesthesia providers when formulating an extubation strategy.
Trial registration: This study was retrospectively registered at clinicaltrials.gov (NCT05361850) on April 23, 2022.
Keywords: Adult anesthesia; Airway complications; Awake extubation; Deep extubation; General endotracheal anesthesia; Randomized controlled trials.
© 2025. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the Naval Medical Center Portsmouth’s Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human subjects. Informed consent was obtained from all research subjects. Our study adhered to the World Medical Association Declaration of Helsinki, with the exception of trial registration before recruitment of the first subject, which was accomplished retrospectively before trial conclusion. Ignorance of the primary investigator, research personnel turnover during the COVID-19 pandemic, and administrative oversight were the root causes of this error. The only significant protocol change made after IRB approval and study initiation was formalizing the anesthesia provider’s discretion to forgo randomization and select an extubation method based on clinically compelling intraoperative events. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Cook TM, Woodall N, Frerk C, Fourth National Audit Project. Major complications of airway management in the UK: results of the fourth National audit project of the Royal college of anaesthetists and the difficult airway society. Part 1: anaesthesia. Br J Anaesth. 2011;106(5):617–31. - PubMed
-
- Asai T, Koga K, Vaughan RS. Respiratory complications associated with tracheal intubation and extubation. Br J Anaesth. 1998;80(6):767–75. - PubMed
-
- Daley MD, Norman PH, Coveler LA. Tracheal extubation of adult surgical patients while deeply anesthetized: a survey of united States anesthesiologists. J Clin Anesth. 1999;11(6):445–52. - PubMed
-
- Nemecek R, Nemecek E, Glaser C, Wallner T, Ratzinger F, Hollinsky C. Impact of two extubation techniques on the intra-abdominal pressure: a preliminary study. Hernia J Hernias Abdom Wall Surg. 2015;19(2):307–11. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
