Assessing inspiratory drive and effort in critically ill patients at the bedside
- PMID: 40745324
- PMCID: PMC12315345
- DOI: 10.1186/s13054-025-05526-0
Assessing inspiratory drive and effort in critically ill patients at the bedside
Abstract
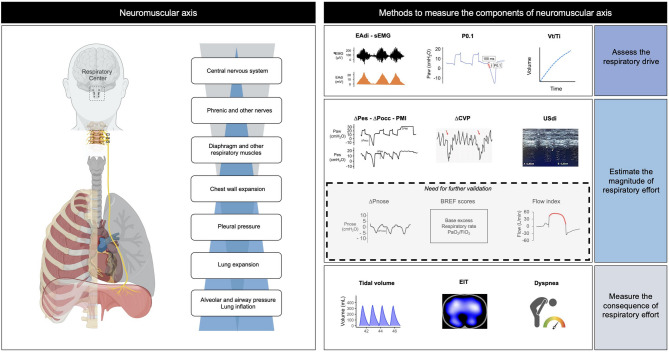
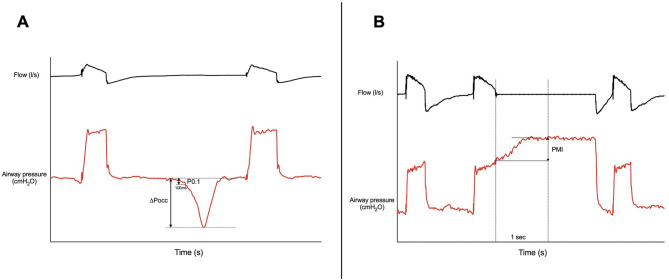
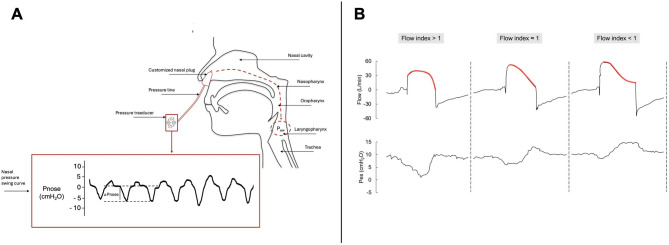
Monitoring inspiratory drive and effort may aid proper selection and setting of respiratory support in patients with acute respiratory failure (ARF), whether they are intubated or not. Although diaphragmatic electrical activity (EAdi) and esophageal manometry can be considered the reference methods for assessing respiratory drive and inspiratory effort, respectively, various alternative techniques exist, each with distinct advantages and limitations. This narrative review provides a comprehensive overview of bedside methods to assess respiratory drive and effort, with a primary focus on patients with ARF. First, EAdi and esophageal manometry are described and discussed as reference techniques. Then, alternative methods are categorized along the neuromechanical pathway from inspiratory drive to muscular effort into three groups: (1) techniques assessing the respiratory drive: airway occlusion pressure (P0.1), mean inspiratory flow (Vt/Ti) and respiratory muscle surface electromyography (sEMG); (2) techniques assessing the respiratory muscle effort: whole-breath occlusion pressure (ΔPocc), pressure-muscle index (PMI), nasal pressure swing (ΔPnose), diaphragm ultrasonography (USdi), central venous pressure swing (ΔCVP), breathing effort (BREF) models, and flow index; (3) techniques and clinical parameters assessing the consequences of effort: tidal volume (Vt), electrical impedance tomography (EIT), dyspnea. For each, we summarize the physiological rationale, measurement methodology, interpretation of results, and key limitations.
Supplementary Information: The online version contains supplementary material available at 10.1186/s13054-025-05526-0.
Keywords: Acute respiratory failure; Esophageal pressure; Inspiratory effort; Patient self-inflicted lung injury; Respiratory monitoring; Ventilator-induced diaphragm dysfunction..
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: RT and EC declares patent N. 102021000007478 “APPARATO PER IL RILEVAMENTO ED IL MONITORAGGIO DELLA PRESSIONE NASALE” released on March 28th, 2023 by the Italian Ministry of Enterprises and Made in Italy. RT and EC are co-founders of IREC ltd (VAT 02959080355), (Reggio Emilia, Italy). Outside of this work, AJ has received research funding (paid to the institution) from ZonMw, Pulmotech B.V., Health~Holland, Liberate Medical, the Netherlands eScience center.
Figures