

Syndrome of inappropriate antidiuretic hormone secretion in a patient with colon cancer using CAPOX plus bevacizumab therapy: a case report
- PMID: 40745570
- PMCID: PMC12312542
- DOI: 10.1186/s40780-025-00476-9
Syndrome of inappropriate antidiuretic hormone secretion in a patient with colon cancer using CAPOX plus bevacizumab therapy: a case report
Abstract
Background: Hyponatremia is an electrolyte abnormality that is often caused by the syndrome of inappropriate antidiuretic hormone secretion (SIADH) and frequently encountered in the field of oncology. Although SIADH is a known complication of certain chemotherapeutic agents, its occurrence with oxaliplatin is rare. We report a case of SIADH in a patient with colon cancer who was undergoing treatment comprising capecitabine and oxaliplatin (CAPOX) plus bevacizumab.
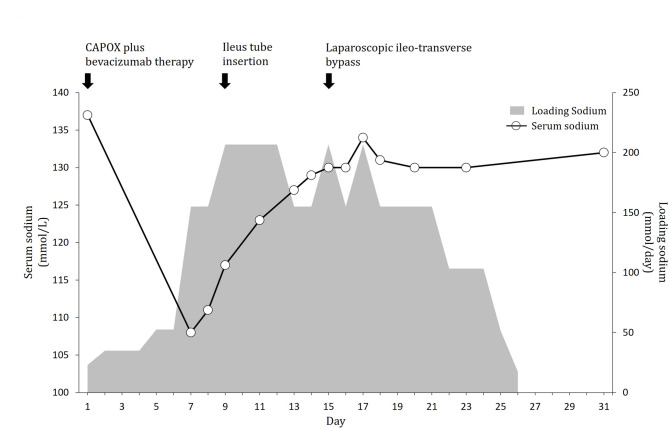
Case presentation: A 70-year-old man with stage cT4bN2M0 colon cancer underwent chemotherapy with CAPOX plus bevacizumab. On day 7 of treatment, the patient developed severe hyponatremia (serum sodium level, 108 mmol/L) accompanied by nausea and ileus. Laboratory test results were consistent with SIADH, including low serum osmolality, elevated urine osmolality, elevated sodium concentration, and elevated antidiuretic hormone levels. The condition improved with 3% saline infusion and fluid restriction. No other underlying causes, such as central nervous system lesions or adrenal or thyroid dysfunction, were identified. CAPOX-induced SIADH was diagnosed based on clinical findings and the exclusion of other etiologies. Transition to second-line therapy was performed without SIADH recurrence.
Conclusions: Oxaliplatin-based regimens may rarely induce SIADH. Clinicians should be vigilant of electrolyte disturbances during chemotherapy and promptly manage hyponatremia to avoid severe complications.
Keywords: Bevacizumab; Capecitabine; Colon cancer; Hyponatremia; Oxaliplatin; Syndrome of inappropriate antidiuretic hormone secretion.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval was waived for this case report as it does not meet the criteria for human subject research requiring Institutional Review Board of Fukuoka University Chikushi Hospital review. Consent for publication: Consent for the publication of this case report was obtained from the patient’s wife as a representative because the patient was no longer alive at the time of submission to this journal. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Chronic Hypertonic Hyponatremia in Lung Cancer: The Utility of the Osmolar Gap.Cureus. 2025 Jul 30;17(7):e89100. doi: 10.7759/cureus.89100. eCollection 2025 Jul. Cureus. 2025. PMID: 40747198 Free PMC article.
-
The use of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer: systematic review and economic evaluation.Health Technol Assess. 2008 May;12(15):iii-ix, xi-162. doi: 10.3310/hta12150. Health Technol Assess. 2008. PMID: 18462574
-
Interventions for chronic non-hypovolaemic hypotonic hyponatraemia.Cochrane Database Syst Rev. 2018 Jun 28;6(6):CD010965. doi: 10.1002/14651858.CD010965.pub2. Cochrane Database Syst Rev. 2018. PMID: 29953167 Free PMC article.
-
Severe hyponatremia in a mild COVID-19 patient: diagnostic challenges of SIADH and adrenal insufficiency.CEN Case Rep. 2025 Jun;14(3):413-420. doi: 10.1007/s13730-025-00995-2. Epub 2025 May 2. CEN Case Rep. 2025. PMID: 40314920 Free PMC article.
-
Antipsychotic-induced hyponatraemia: a systematic review of the published evidence.Drug Saf. 2010 Feb 1;33(2):101-14. doi: 10.2165/11319070-000000000-00000. Drug Saf. 2010. PMID: 20082537
References
-
- Palmer BF, Gates JR, Lader M. Causes and management of hyponatremia. Ann Pharmacother. 2003; 37: 1694–702. Available from: 10.1345/aph.1D105 - PubMed
-
- Raftopoulos H. Diagnosis and management of hyponatremia in cancer patients. Support Care Cancer. 2007; 15: 1341–7. Available from: 10.1007/s00520-007-0309-9 - PubMed
-
- Berghmans T. Hyponatremia related to medical anticancer treatment. Support Care Cancer. 1996; 4: 341–350. Available from: 10.1007/BF01788840 - PubMed
-
- Iyer AV, Krasnow SH, Dufour DR, Arcenas AS. Sodium-wasting nephropathy caused by cisplatin in a patient with small-cell lung cancer. Clin. Lung Cancer. 2003, 5, 187–9. Available from: 10.3816/CLC.2003.n.033 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
