

Diminished Cerebral Oxygen Extraction and Metabolic Rate in Neonates With Hypoxic Ischemic Encephalopathy
- PMID: 40747539
- PMCID: PMC12483023
- DOI: 10.1161/STROKEAHA.125.051107
Diminished Cerebral Oxygen Extraction and Metabolic Rate in Neonates With Hypoxic Ischemic Encephalopathy
Abstract
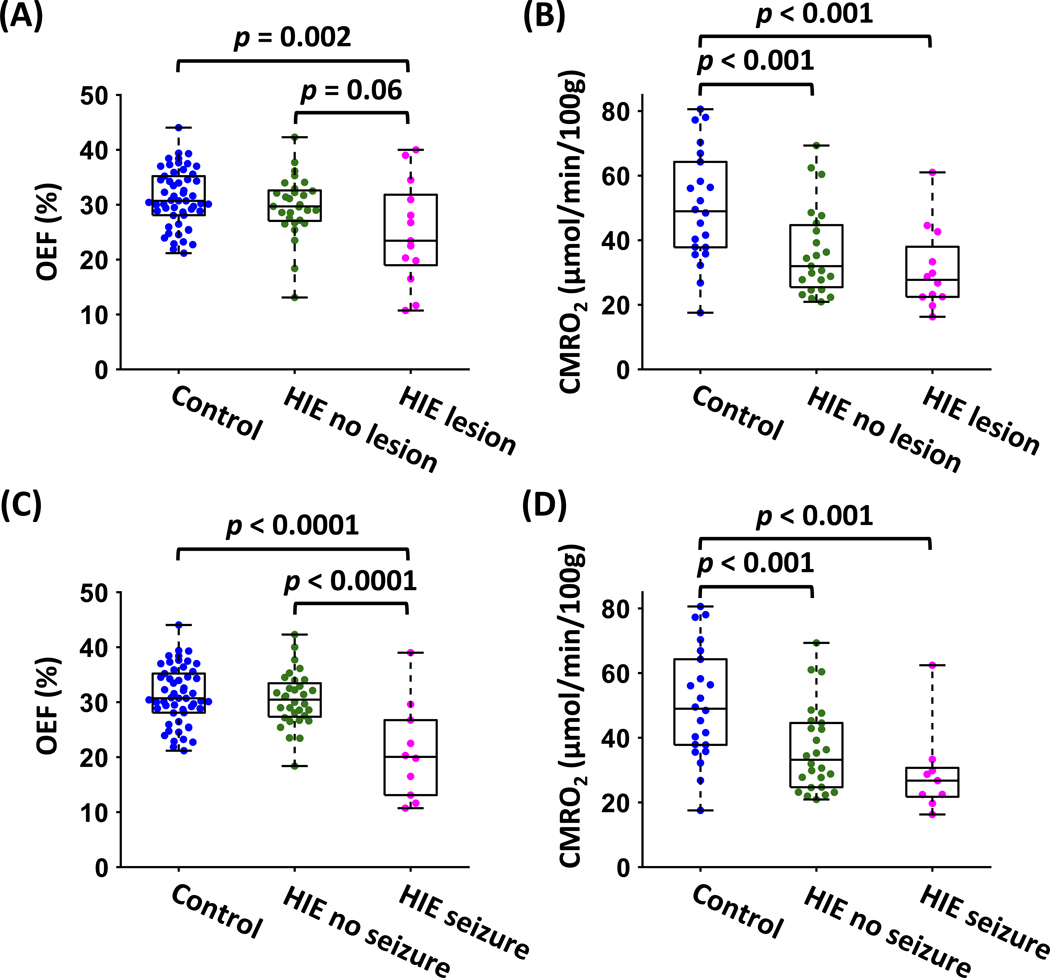
Background: Hypoxic ischemic encephalopathy (HIE), which is associated with perinatal disruption of cerebral oxygen supply and utilization, is a leading cause of neonatal mortality and severe neurological impairment in childhood. The present study investigated whether key physiological parameters of cerebral oxygen utilization, specifically oxygen extraction fraction (OEF), cerebral blood flow, and cerebral metabolic rate of oxygen (CMRO2), were altered in neonates with HIE, and whether these parameters were associated with clinical indices.
Methods: In this case-control study, neonates with HIE and healthy control newborns were enrolled from the Johns Hopkins Children's Center and the Children's Hospital at the University of Maryland Medical Center. The brain's hemodynamic and metabolic parameters of OEF, cerebral blood flow, and CMRO2 were measured with noncontrast magnetic resonance imaging and were compared between neonates with HIE and controls. We studied the relationships between the brain's physiological parameters and the presence of structural brain lesions and Apgar scores in neonates with HIE and controls. Additionally, we investigated the associations between these physiological parameters and the length of stay in the neonatal intensive care unit among neonates with HIE.
Results: Forty-two neonates with HIE and 54 control neonates were included. Neonates with HIE exhibited lower OEF (control, 31.2±5.2% versus HIE, 28.3±7.3%; P=0.02) and CMRO2 (control, 50.4±17.3 μmol/min per 100 grams versus HIE, 34.5±13.5 μmol/min per 100 gram; P<0.0001) compared with control neonates, whereas cerebral blood flow showed no significant difference (control, 15.9±3.9 mL/min per 100 grams versus HIE, 15.2±4.6 mL/min per 100 grams; P=0.61). OEF and CMRO2 were correlated with 1-minute and 5-minute Apgar scores (P<0.05). Among neonates with HIE, lower OEF was associated with a longer neonatal intensive care unit stay (P=0.003).
Conclusions: These findings suggest that cerebral oxygen utilization is compromised in neonates with HIE. The physiological parameters of OEF and CMRO2 may serve as useful biomarkers for evaluating cerebral injury and planning treatment in HIE.
Keywords: brain injuries; hypoxia-ischemia, brain; infant, newborn; oxygen consumption.
Conflict of interest statement
Dr Golden received compensation from Elsevier for other services, royalty for Associate Editor of 5-Minute Pediatric Consult, and compensation from MJH Life Sciences for other services. Dr Northington received grants from the National Institutes of Health Office of the Director. The other authors report no conflicts.
Figures





References
-
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. doi: 10.1016/S0140-6736(14)61682-2 - DOI - PMC - PubMed
-
- Jacobs SE, Morley CJ, Inder TE, Stewart MJ, Smith KR, McNamara PJ, Wright IM, Kirpalani HM, Darlow BA, Doyle LW, et al. Whole-body hypothermia for term and near-term newborns with hypoxic-ischemic encephalopathy: a randomized controlled trial. Arch Pediatr Adolesc Med. 2011;165:692–700. doi: 10.1001/archpediatrics.2011.43 - DOI - PubMed
-
- Dehaes M, Aggarwal A, Lin PY, Rosa Fortuno C, Fenoglio A, Roche-Labarbe N, Soul JS, Franceschini MA, Grant PE. Cerebral oxygen metabolism in neonatal hypoxic ischemic encephalopathy during and after therapeutic hypothermia. J Cereb Blood Flow Metab. 2014;34:87–94. doi: 10.1038/jcbfm.2013.165 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
