

Abdominal organ injury in cardiac arrest: Systematic literature review
- PMID: 40749012
- PMCID: PMC12316268
- DOI: 10.1371/journal.pone.0329164
Abdominal organ injury in cardiac arrest: Systematic literature review
Abstract
Background: Both cardiopulmonary resuscitation (CPR) and ischaemia could lead to abdominal organ injury. However, the importance of abdominal injury in cardiac arrest remains uncertain. We aimed to systematically review indexed literature to describe incidence of abdominal injury after non-traumatic cardiac arrest and associations with outcome.
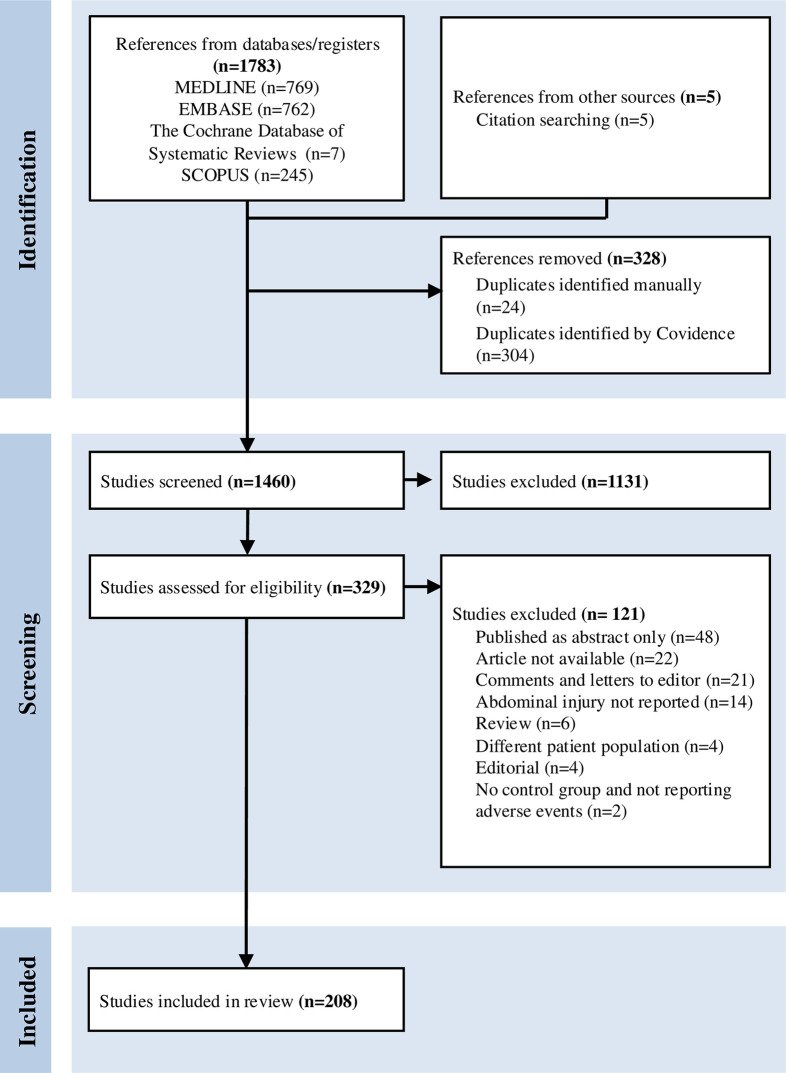
Methods: We searched MEDLINE/PubMed, Embase, The Cochrane Database of Systematic Reviews and Scopus up to 12th September 2024 for studies reporting differences in outcomes between patients with and without abdominal injury, and all studies reporting abdominal adverse events after cardiac arrest. Two independent reviewers screened articles for eligibility. One reviewer extracted data and assessed risk of bias using the Critical Appraisal Skills Programme checklist. Injuries were defined as traumatic or ischaemic, either in the studies or otherwise by the reviewers. Results were summarized and presented in tables and Forest plots. We followed the PRISMA guidelines, and registered the study in PROSPERO.
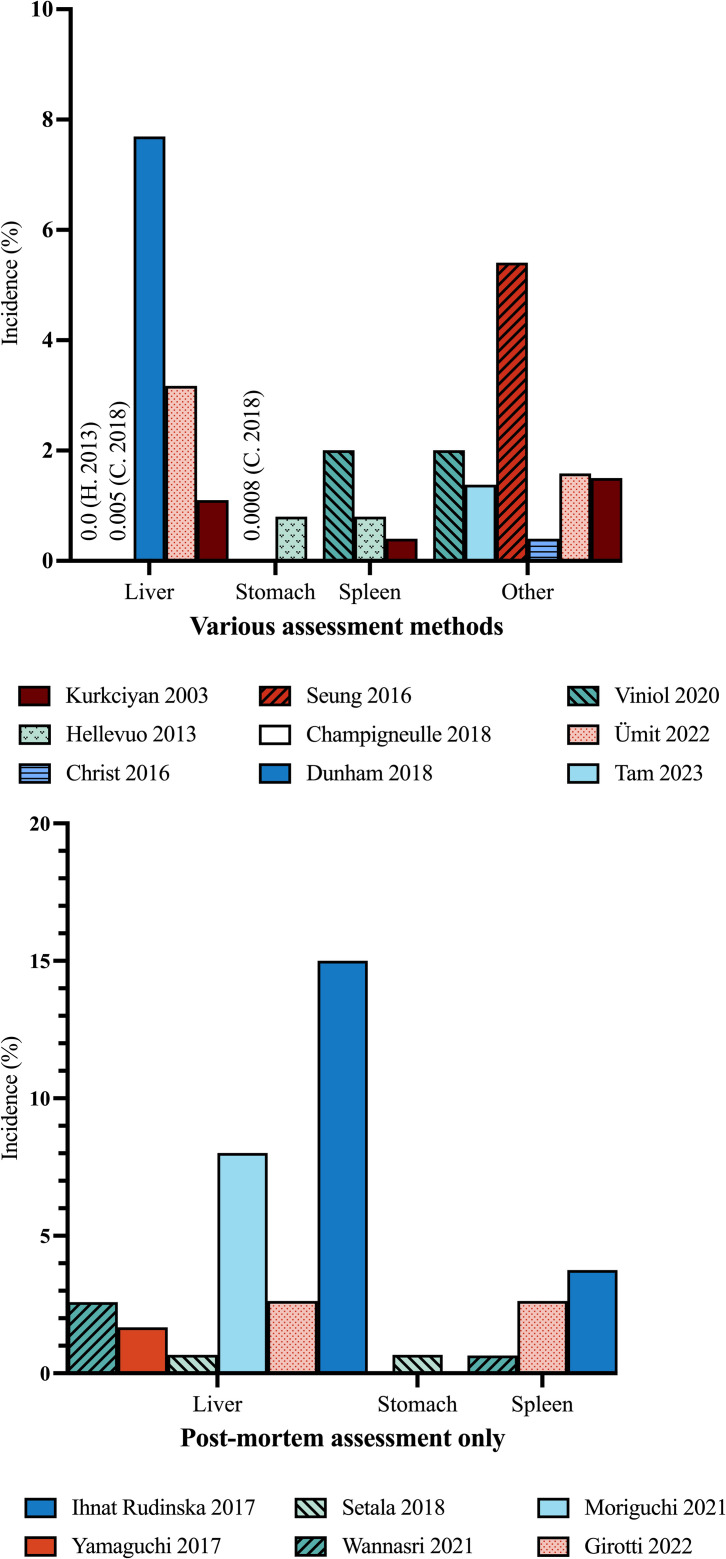
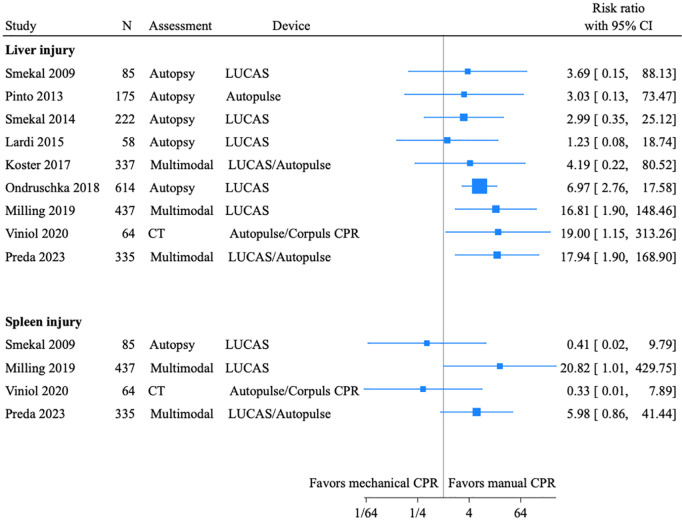
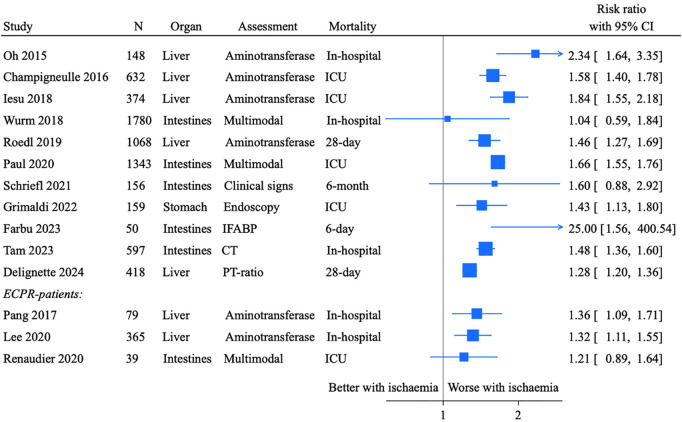
Results: We included 68 studies and 140 case reports. Most studies were single-centre. Quantitative synthesis of evidence was not feasible given high heterogeneity and risk of bias. Traumatic injuries affected mostly liver and spleen, with incidences from 0% to 15%, reaching 29% in one study of mechanical chest compressions. Life-threatening injuries were uncommon. The incidence of ischaemic injury was dependent on assessment method; 7% to 28% had liver injury, 0.7% to 2.5% was diagnosed with non-occlusive mesenteric ischaemia, 82% to 100% had intestinal injury measured by biomarkers. Ischaemic injuries were associated with mortality.
Conclusion: In this comprehensive review of abdominal injuries following cardiac arrest, CPR-related traumatic injuries were uncommon, but should be considered in patients with unexplained clinical deterioration. Ischaemic injury incidence ranged from 0.7% to 100%, and was consistently associated with mortality. Whether abdominal ischaemia independently contributes to poor outcomes remains unresolved and warrants further investigation. PROSPERO ID: CRD42022311508.
Copyright: © 2025 Hoftun Farbu et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Continuous chest compression versus interrupted chest compression for cardiopulmonary resuscitation of non-asphyxial out-of-hospital cardiac arrest.Cochrane Database Syst Rev. 2017 Mar 27;3(3):CD010134. doi: 10.1002/14651858.CD010134.pub2. Cochrane Database Syst Rev. 2017. PMID: 28349529 Free PMC article.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Eliciting adverse effects data from participants in clinical trials.Cochrane Database Syst Rev. 2018 Jan 16;1(1):MR000039. doi: 10.1002/14651858.MR000039.pub2. Cochrane Database Syst Rev. 2018. PMID: 29372930 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
