

Unexpected Ventricular Fibrillation During a Cardiovascular Magnetic Resonance Examination Documented With Simultaneous Quantitative Myocardial Perfusion
- PMID: 40750155
- PMCID: PMC12441519
- DOI: 10.1016/j.jaccas.2025.104027
Unexpected Ventricular Fibrillation During a Cardiovascular Magnetic Resonance Examination Documented With Simultaneous Quantitative Myocardial Perfusion
Abstract
Background: Unexpected life-threatening arrhythmias, even when occurring in hospital, are frequently ill documented, hindering a proper understanding of their mechanism.
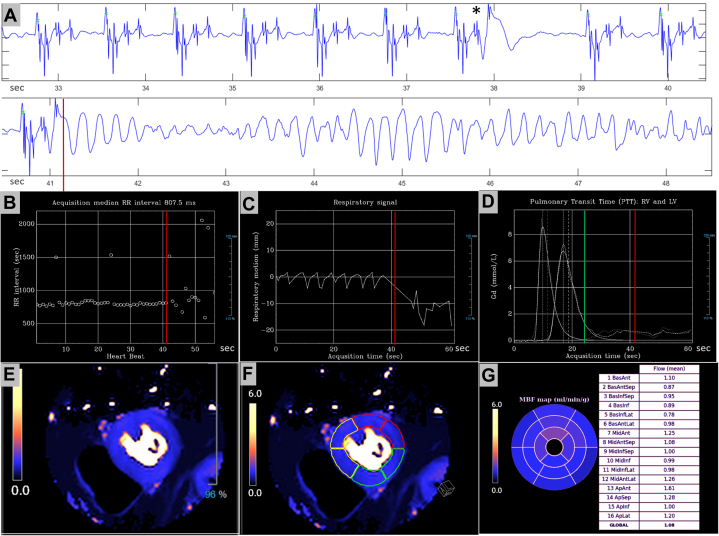
Case summary: We present a patient with coronary artery disease who developed an episode of ventricular fibrillation during a cardiovascular magnetic resonance examination. The arrhythmia appeared immediately after the injection of a contrast agent during a quantitative myocardial perfusion sequence at rest, with no stressor agent involved.
Discussion: To our knowledge, this is the first episode of ventricular fibrillation documented with simultaneous electrocardiographic, physiological recordings, and quantitative myocardial perfusion data. Such unique information allowed for a comprehensive analysis of the sequence of facts preceding the final arrhythmia and, in consequence, provided a well-reasoned conclusion on its mechanism.
Keywords: cardiac magnetic resonance; contrast agent; perfusion; ventricular fibrillation.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Vidorreta is an employee of Siemens Healthineers, Madrid, Spain. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
-
- Power S., Talbot N., Kucharczyck W., Mandell D.M. Allergic-like reactions to the MR imaging contrast agent gadobutrol: a prospective study of 32 991 consecutive injections. Radiology. 2016;281:72–77. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
