

Gross total resection in low-grade and pretreated high-grade invasive growth hormone pituitary adenomas promises favorable outcomes
- PMID: 40751108
- PMCID: PMC12316652
- DOI: 10.1007/s12672-025-03313-5
Gross total resection in low-grade and pretreated high-grade invasive growth hormone pituitary adenomas promises favorable outcomes
Abstract
Introduction: Growth hormone (GH)-secreting pituitary tumors cause serious systemic comorbidities, necessitating the achievement of gross total resection (GTR) and biochemical remission. This study aims to identify predictors of resection status and biochemical remission.
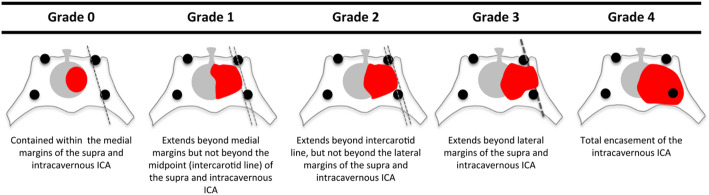
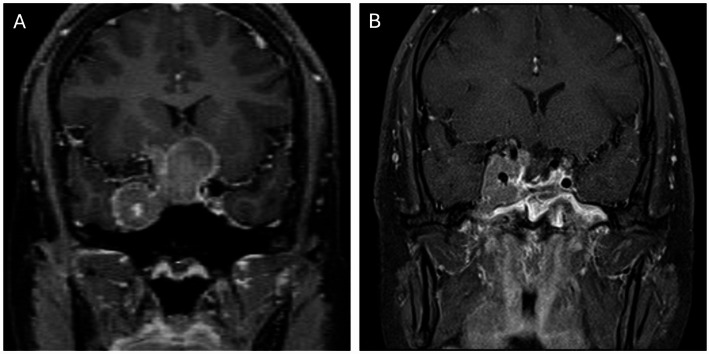
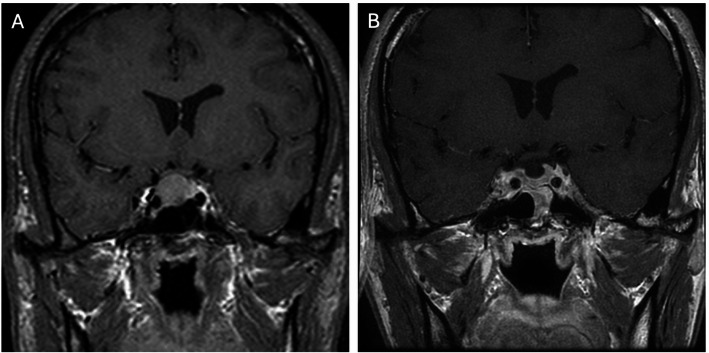
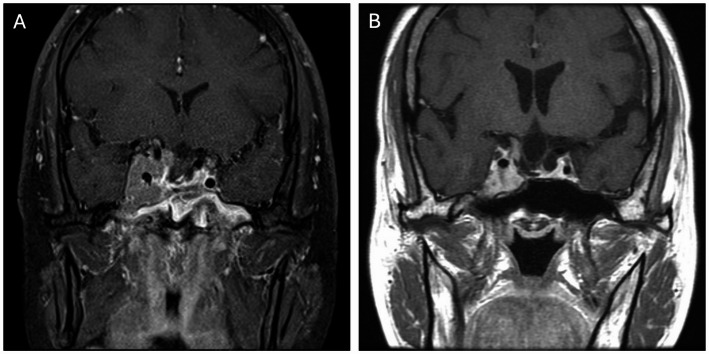
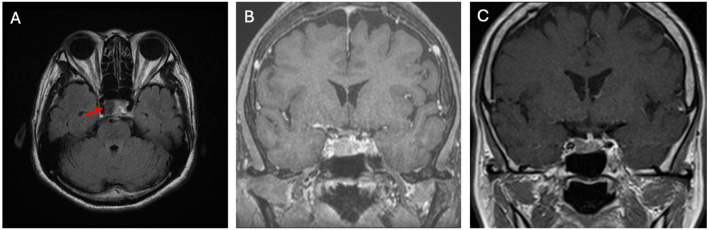
Methods: We retrospectively reviewed the records of 54 GH adenoma patients receiving endoscopic endonasal transsphenoidal approach (EETSA). Medical records and magnetic resonance imaging were reviewed for tumor size, volume, resection status, invasion status, and Knosp and Hardy-Wilson grades. We also classified invasion status into high- and low-grade groups. Biochemical remission was defined as an insulin-like growth factor 1 value within sex- and age-adjusted reference or a random GH level < 1.0 ng/mL.
Results: The degrees of horizontal and vertical invasion based on preoperative Knosp and Hardy-Wilson grade were highly associated with intraoperative resection status (p = 0.0054, 0.0043 and 0.013 respectively). We also found more significant differences between resection status and higher-grade invasion (p = 0.0018, 0.006 and 0.0018, respectively). Hardy-Wilson grades and resection status were significantly associated with biochemical remission (p = 0.0484, 0.0252, and 0.0007, respectively). Although we observed no difference between outcomes with respect to micro- vs. macroadenoma, tumor size and volume were significantly associated with outcomes (p = 0.017, 0.0032, respectively). More significant differences were observed between biochemical remission and higher-grade Hardy-Wilson invasion grade (p = 0.0053 and 0.0075). Multivariate analysis showed that higher-grade Hardy-Wilson invasion correlated with resection status (p = 0.0481 and 0.0125); only resection status was associated with biochemical remission (p = 0.0101).
Conclusions: EETSA remains the best treatment option for GH adenomas. Biochemical remission was highly associated with invasion status and the possibility of achieving GTR. Aggressive resection for low-grade and pretreated high-grade tumors promises favorable outcomes.
Keywords: Biochemical remission; Endoscopic endonasal transsphenoidal approach; GH pituitary adenoma; Knosp and Hardy–Wilson grade; Pre-operative treatment; Resection status.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Institutional Review Board (IRB) of Chang Gung Memorial Hospital (IRB No. 202401326B0). Informed consent was obtained from all individual participants included in the study. The authors affirm that human research participants provided informed consent for publication of their data in the manuscript. Consent for publication: Informed consent was obtained from all individual participants included in the study. Competing interests: The authors declare no competing interests.
Figures

References
-
- Araujo-Castro M, et al. Predictive model of surgical remission in acromegaly: age, presurgical GH levels and Knosp grade as the best predictors of surgical remission. J Endocrinol Invest. 2021;44(1):183–93. - PubMed
-
- Shin SS, et al. Endoscopic endonasal approach for growth hormone secreting pituitary adenomas: outcomes in 53 patients using 2010 consensus criteria for remission. Pituitary. 2013;16(4):435–44. - PubMed
-
- Taghvaei M, et al. Endoscopic endonasal approach to the growth Hormone-Secreting pituitary adenomas: endocrinologic outcome in 68 patients. World Neurosurg. 2018;117:e259–68. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources