

AI enhanced diagnostic accuracy and workload reduction in hepatocellular carcinoma screening
- PMID: 40753139
- PMCID: PMC12318110
- DOI: 10.1038/s41746-025-01892-9
AI enhanced diagnostic accuracy and workload reduction in hepatocellular carcinoma screening
Abstract
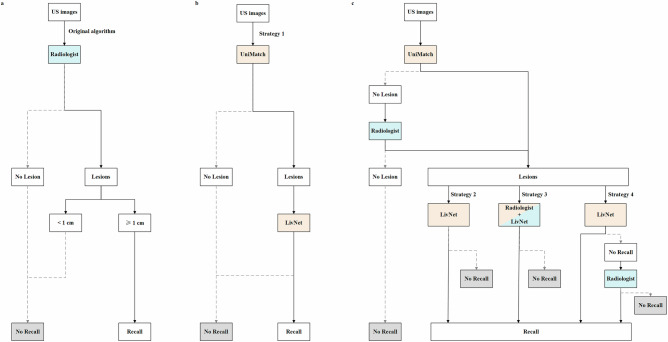
Hepatocellular carcinoma (HCC) ultrasound screening encounters challenges related to accuracy and the workload of radiologists. This retrospective, multicenter study assessed four artificial intelligence (AI) enhanced strategies using 21,934 liver ultrasound images from 11,960 patients to improve HCC ultrasound screening accuracy and reduce radiologist workload. UniMatch was used for lesion detection and LivNet for classification, trained on 17,913 images. Among the strategies tested, Strategy 4, which combined AI for initial detection and radiologist evaluation of negative cases in both detection and classification phases, outperformed others. It not only matched the high sensitivity of original algorithm (0.956 vs. 0.991) but also improved specificity (0.787 vs. 0.698), reduced radiologist workload by 54.5%, and decreased both recall and false positive rates. This approach demonstrates a successful model of human-AI collaboration, not only enhancing clinical outcomes but also mitigating unnecessary patient anxiety and system burden by minimizing recalls and false positives.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures






References
-
- Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J. Clin.10.3322/caac.21834 (2024). - PubMed
-
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol.69, 182–236, (2018). - PubMed
-
- Marrero, J. A. et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatol. (Baltim., Md.)68, 723–750 (2018). - PubMed
-
- Vosshenrich, J. et al. Quantifying Radiology Resident Fatigue: Analysis of Preliminary Reports. Radiology298, 632–639 (2021). - PubMed
Grants and funding
- 2024A1515220047/Science Fund for Distinguished Young Scholars of Guangdong Province
- 2024A1515220047/Science Fund for Distinguished Young Scholars of Guangdong Province
- 2024A1515220047/Science Fund for Distinguished Young Scholars of Guangdong Province
- 82272076/National Natural Science Foundation of China
- 82371983/National Natural Science Foundation of China
LinkOut - more resources
Full Text Sources
