

Acute Uterine Torsion Masquerading as Fibroid Degeneration in a High-Risk Pregnancy: A Case of Diagnostic Surprise
- PMID: 40755576
- PMCID: PMC12315048
- DOI: 10.7759/cureus.87156
Acute Uterine Torsion Masquerading as Fibroid Degeneration in a High-Risk Pregnancy: A Case of Diagnostic Surprise
Abstract
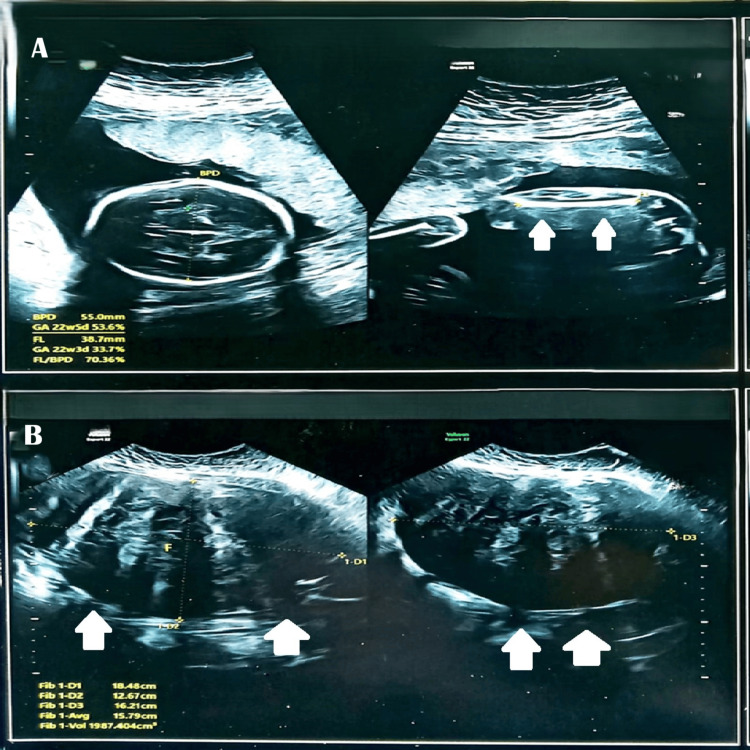
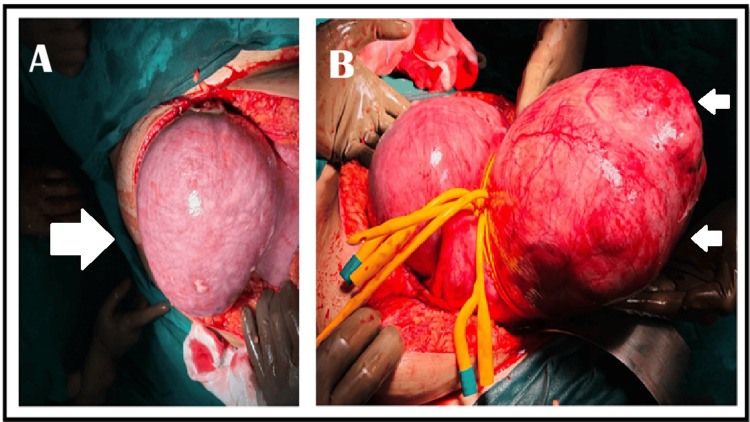
Uterine torsion during pregnancy is a rare and life-threatening condition that is frequently misdiagnosed due to nonspecific symptoms and imaging limitations. This case report describes a 32-year-old third gravida (G3, P0+2) with recurrent pregnancy loss, having a 16.9 cm uterine fibroid and hypertrophic cardiomyopathy (managed with bisoprolol), who presented at 24 weeks with severe abdominal pain. Although her vitals were stable, a markedly elevated C-reactive protein (CRP) (245 mg/dL) raised concern for acute pathology. Initial ultrasound incorrectly localized the fibroid to the left, but exploratory laparotomy revealed a 180-degree uterine torsion with contralateral fibroid position, revising the diagnosis from fibroid degeneration to this rare emergency, leading to detorsion and myomectomy. At 30 weeks' gestation, cervical insufficiency (a short cervix measuring 0.5 cm with funneling) was successfully managed with an Arabin pessary and weekly 500 mg injections of hydroxyprogesterone, prolonging the pregnancy to 34 weeks and resulting in an outlet forceps delivery of a healthy 1.9 kg infant. This case highlights the importance of surgical exploration when clinical suspicion contradicts imaging findings, the feasibility of pregnancy-preserving surgery for uterine torsion, and the effectiveness of combined mechanical-hormonal therapy for cervical insufficiency following complex uterine interventions. Multidisciplinary care was critical to manage overlapping high-risk factors, including fibroids, cardiac disease, and preterm cervical changes, ultimately leading to a favorable outcome.
Keywords: arabin pessary; myomectomy in pregnancy; preterm labor and obstetric care; uterine fibroid in pregnancy; uterine torsion.
Copyright © 2025, Samanta et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Uterine torsion: a review with critical considerations for the obstetrician and gynecologist. Liang R, Gandhi J, Rahmani B, Khan SA. Transl Res Anat. 2020;21:100084.
-
- Differential diagnosis of uterine leiomyoma torsion mimicking ovarian torsion in a second trimester of pregnancy: a case report. Kim HJ, Lee J, Lee HJ. https://doi.org/10.2147/IJWH.S385321. Int J Womens Health. 2022;14:1777–1782. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous