

Acute Liver Failure Secondary to Primary Large B-cell Lymphoma Complicated by Malignancy-related Hemophagocytic Syndrome: A Case Report
- PMID: 40755712
- PMCID: PMC12318538
- DOI: 10.7759/cureus.87288
Acute Liver Failure Secondary to Primary Large B-cell Lymphoma Complicated by Malignancy-related Hemophagocytic Syndrome: A Case Report
Abstract
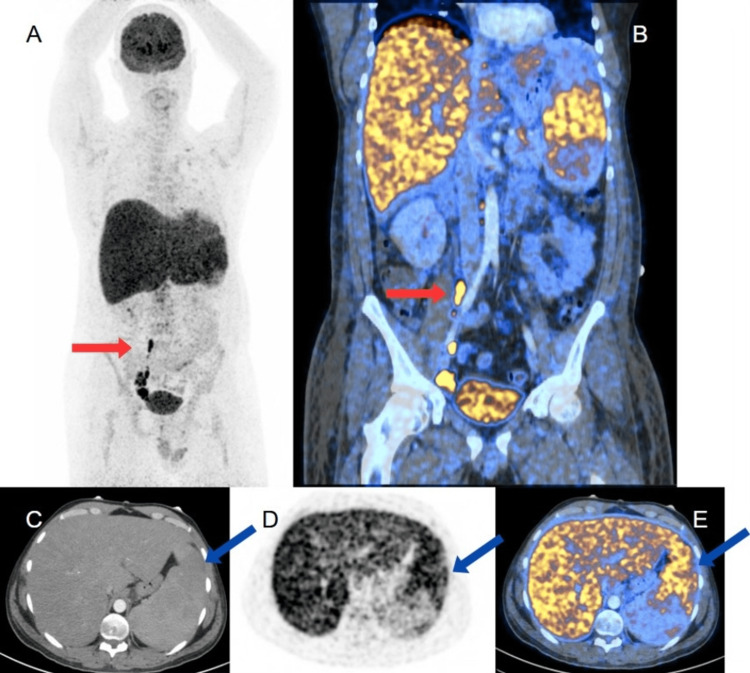
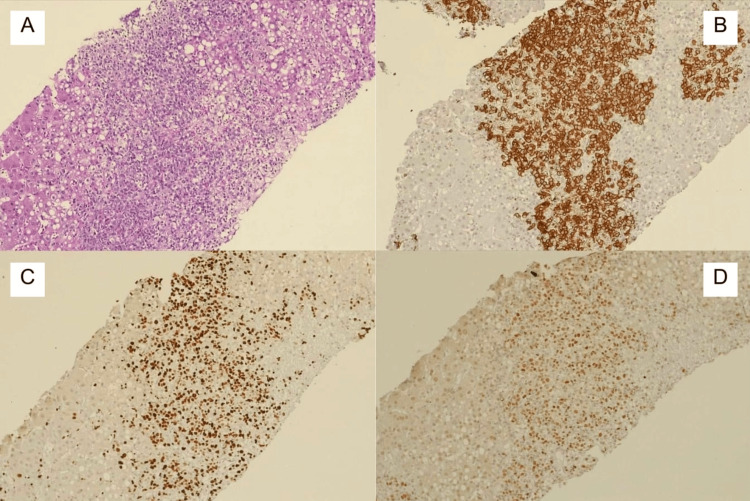
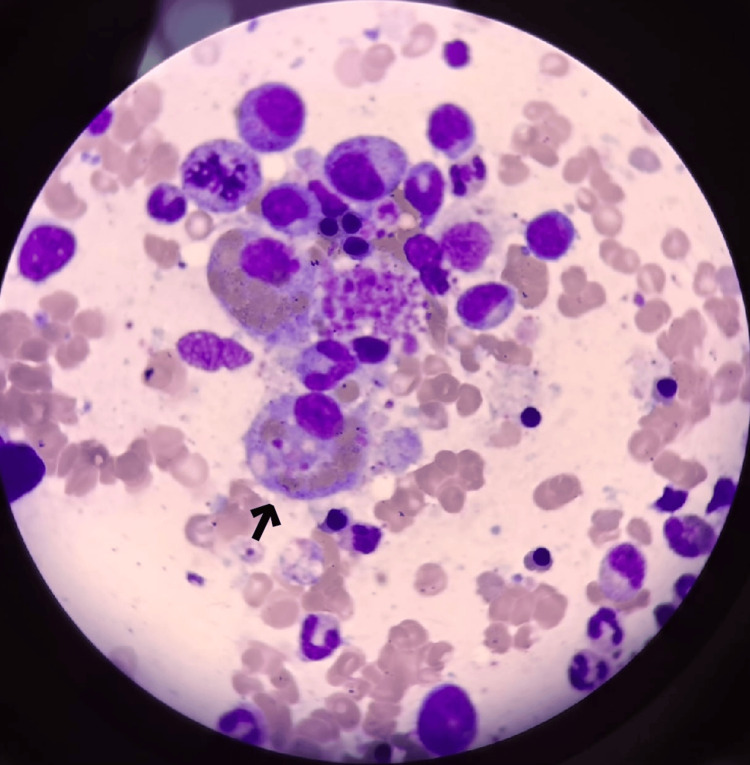
Acute liver failure is a catastrophic condition characterized by the sudden and severe impairment of hepatic function. We report the case of a 36-year-old patient who presented with significant dehydration, generalized jaundice, evidence of hepatic encephalopathy, generalized edema with abdominal distension, and hepatosplenomegaly. A liver biopsy was performed, yielding the final diagnosis of primary large B-cell lymphoma. Subsequently, a bone marrow aspirate and biopsy were performed, confirming the diagnosis of hemophagocytic syndrome. The patient was managed with R-CHOEP (rituximab, cyclophosphamide, doxorubicin, vincristine, etoposide, prednisone) chemotherapy. After 21 days, the patient was successfully discharged to continue treatment on an outpatient basis.
Keywords: acute liver failure (alf); diffuse large b cell lymphoma (dlbcl); hemophagocytic syndrome (hs); lymphoma; non-hodgkin lymphoma (nhl).
Copyright © 2025, Rivera Tapia et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Treating newly diagnosed Diffuse Large B-cell Lymphoma in the elderly patient with R-mini-CHOP: A single centre analytical retrospective observational study.Med J Malaysia. 2025 May;80(3):307-312. Med J Malaysia. 2025. PMID: 40437719
-
[Positron emission tomography-negative hemophagocytic lymphohistiocytosis in two patients with aggressive B-cell lymphoma].Inn Med (Heidelb). 2025 Aug 4. doi: 10.1007/s00108-025-01957-7. Online ahead of print. Inn Med (Heidelb). 2025. PMID: 40760333 German.
-
Sodium 2-Mercaptoethanesulfonate (MESNA), Ifosfamide, Mitoxantrone, and Etoposide (MINE) in Transplant-Ineligible Relapsed/Refractory Diffuse Large B-Cell Lymphoma: Is the Old Regimen Still Gold?Cureus. 2025 Jul 1;17(7):e87128. doi: 10.7759/cureus.87128. eCollection 2025 Jul. Cureus. 2025. PMID: 40755587 Free PMC article.
-
Rituximab (MabThera) for aggressive non-Hodgkin's lymphoma: systematic review and economic evaluation.Health Technol Assess. 2004 Sep;8(37):iii, ix-xi, 1-82. doi: 10.3310/hta8370. Health Technol Assess. 2004. PMID: 15361313
-
Rituximab for the first-line treatment of stage III-IV follicular lymphoma (review of Technology Appraisal No. 110): a systematic review and economic evaluation.Health Technol Assess. 2012;16(37):1-253, iii-iv. doi: 10.3310/hta16370. Health Technol Assess. 2012. PMID: 23021127
References
-
- Primary hepatic large B-cell lymphoma. Arker SH, Chen A. Hum Path Rep. 2022;28:300653.
-
- Acute liver failure secondary to diffuse large B-cell lymphoma discovered on explant pathology. Hughes B, McGinnis T, Hibbert J, Jackson W. Ann Intern Med Clin Cases. 2024;3
Publication types
LinkOut - more resources
Full Text Sources