

Minimally invasive techniques versus opioids in patients with unresectable pancreatic cancer: a systematic review and meta-analysis of randomised controlled trials
- PMID: 40755737
- PMCID: PMC12314671
- DOI: 10.21037/tgh-24-141
Minimally invasive techniques versus opioids in patients with unresectable pancreatic cancer: a systematic review and meta-analysis of randomised controlled trials
Abstract
Background: Pancreatic cancer (PC) has a low chance of resection, and a consistent burden of disease, with pain greatly impacting the quality of life (QoL). We aim to find the most efficient method to treat pain in patients with unresectable PC.
Methods: Our study was registered on PROSPERO (CRD42023477094). On the 29th of October 2023, a systematic search was performed, including only randomised controlled trials (RCTs) reporting on patients with unresectable PC-associated pain, QoL, survival, analgesics use, and adverse events (AEs). Different random-effects meta-analyses were performed on the Visual Analog Scale (VAS) and AEs. Survival curves of treatments were estimated based on individual patients' data from the reported Kaplan-Meier curves.
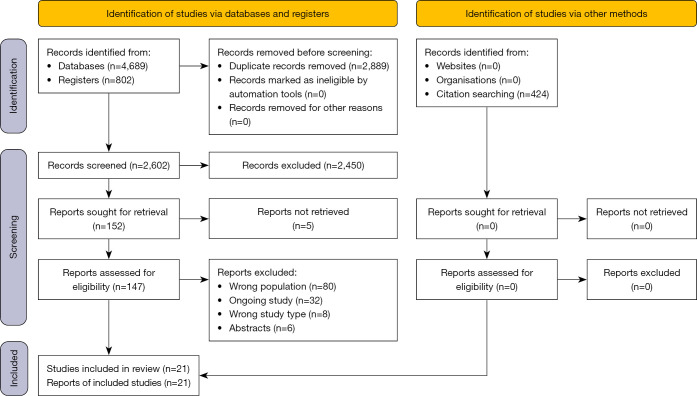
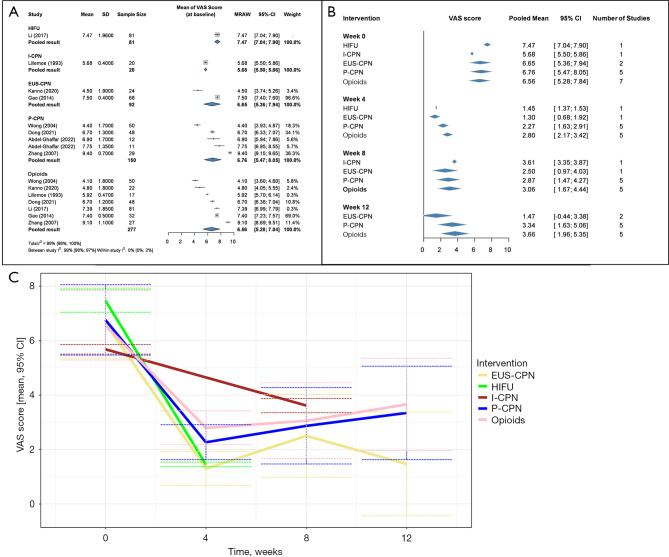
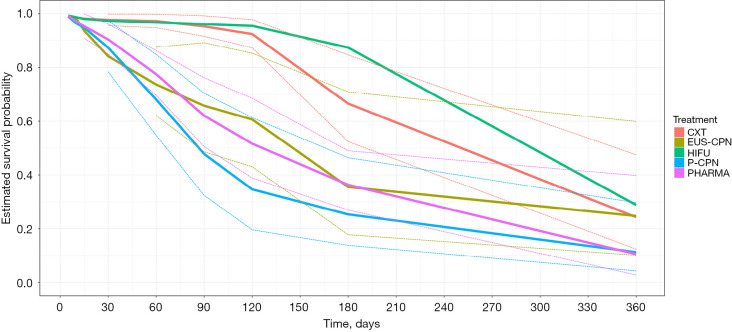
Results: Twenty-one RCTs were eligible. At 4 weeks from a moderate to severe baseline pain level, the VAS score decreased to 2.27 [95% confidence interval (CI): 1.63-2.91] with percutaneous celiac plexus neurolysis (P-CPN), and 2.80 (95% CI: 2.17-3.42) with opioids, while in individual studies to 1.30 (95% CI: 0.68-1.92) with endoscopic ultrasound-guided celiac plexus neurolysis (EUS-CPN), and 1.45 (95% CI: 1.37-1.53) with high-intensity focused ultrasound (HIFU). At 8 and 12 weeks, there was an increase in pain scores for all treatment groups. AEs associated with interventional techniques were transient, the most common being diarrhoea, haemodynamic changes, and procedure-related pain. The median survival time in days was 126.22 (95% CI: 87.21-165.31) for opioids and 86.71 (95% CI: 62.45-136.88) for P-CPN.
Conclusions: Interventional techniques reduce pain and opioid use with few adverse effects; they should be considered more often and earlier in the management of patients with unresectable PC.
Keywords: Adenocarcinoma; Visual Analog Scale (VAS); celiac plexus neurolysis (CPN); high-intensity focused ultrasound (HIFU); pain.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tgh.amegroups.com/article/view/10.21037/tgh-24-141/coif). All authors report that funding was provided by the Centre for Translational Medicine, Semmelweis University. B.T. reports additional funding provided by the New National Excellence Program of the Ministry for Innovation and Technology from the source of the National Research, Development, and Innovation Fund (No. ÚNKP-23-3-II-PTE-1996). The authors have no other conflicts of interest to declare.
Figures
Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Levothyroxine or minimally invasive therapies for benign thyroid nodules.Cochrane Database Syst Rev. 2014 Jun 18;2014(6):CD004098. doi: 10.1002/14651858.CD004098.pub2. Cochrane Database Syst Rev. 2014. PMID: 24941398 Free PMC article.
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Sympathetic nerve blocks for persistent pain in adults with inoperable abdominopelvic cancer.Cochrane Database Syst Rev. 2024 Jun 6;6(6):CD015229. doi: 10.1002/14651858.CD015229.pub2. Cochrane Database Syst Rev. 2024. PMID: 38842054 Free PMC article.
References
-
- Cancer Stat Facts: Pancreatic Cancer. Available online: https://seer.cancer.gov/statfacts/html/pancreas.html
-
- Westermann A, Matrisian LM, Rahib L. The need for improvement in the management of fatigue, depression and pain in pancreatic cancer. J Clin Oncol 2019;37:429.
LinkOut - more resources
Full Text Sources