

Obstructive Ureteral Metastasis From Prostate Cancer
- PMID: 40756077
- PMCID: PMC12316810
- DOI: 10.1002/ccr3.70753
Obstructive Ureteral Metastasis From Prostate Cancer
Abstract
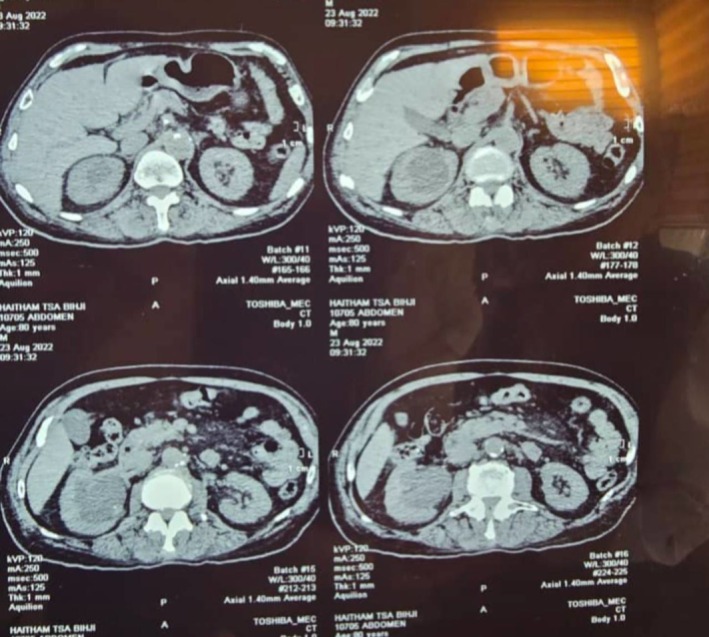
Prostate cancer is the second most common malignancy in males, primarily associated with risk factors such as age, ethnicity, obesity, and family history. While metastases commonly involve lymph nodes, bones, and the liver, ureteral metastasis is exceedingly rare. Ureteral obstruction due to metastatic prostate cancer can lead to hydronephrosis, often requiring ureteroscopy for diagnosis and management. However, persistent symptoms may necessitate exploratory surgery. An 82-year-old Arab male with a history of Gleason 4 + 4 = 8 prostate adenocarcinoma (initially managed with hormonal therapy and surgical castration) presented with right back pain. Imaging revealed stage 4 hydronephrosis, initially attributed to a ureteral stone. Ureteroscopy identified obstructing ureteral tumors instead, with biopsy confirming well-differentiated adenocarcinoma of prostatic origin. Due to persistent obstruction and confirmed malignancy, a right nephroureterectomy was performed. Histopathology demonstrated extensive ureteral involvement (16 cm) with vascular and perineural invasion but no distant metastasis on postoperative PET-CT. This case underscores the diagnostic challenge of ureteral metastasis in prostate cancer, often mimicking benign conditions like ureteral stones. Despite successful local surgical control, the tumor's aggressive features necessitate long-term surveillance and continued hormonal therapy. High clinical suspicion for metastasis is crucial in high-risk prostate cancer patients presenting with obstructive uropathy, even in the absence of significantly elevated PSA. This report highlights the importance of a stepwise diagnostic approach and the need for prompt intervention in such rare presentations.
Keywords: hydronephrosis; metastasis; prostate cancer; ureter stones; ureteral metastasis; ureteral obstruction.
© 2025 The Author(s). Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
