

Association between glycemic control and hepatocellular carcinoma risk in people with type 2 diabetes, stratified by chronic hepatitis B or C infection
- PMID: 40756178
- PMCID: PMC12317228
- DOI: 10.1177/17562848251356198
Association between glycemic control and hepatocellular carcinoma risk in people with type 2 diabetes, stratified by chronic hepatitis B or C infection
Abstract
Background: Chronic viral hepatitis is a major risk factor for hepatocellular carcinoma (HCC). Though diabetes is another risk of HCC, it remains indeterminant as to whether glycemic burden in individuals with type 2 diabetes (T2D) should be differentially managed according to the presence of chronic hepatitis B virus (HBV) or hepatitis C virus (HCV).
Objectives: To evaluate the association between glycemic burden and HCC risk in individuals with T2D, stratified by viral hepatitis status, including HBV and HCV.
Design: Retrospective cohort study.
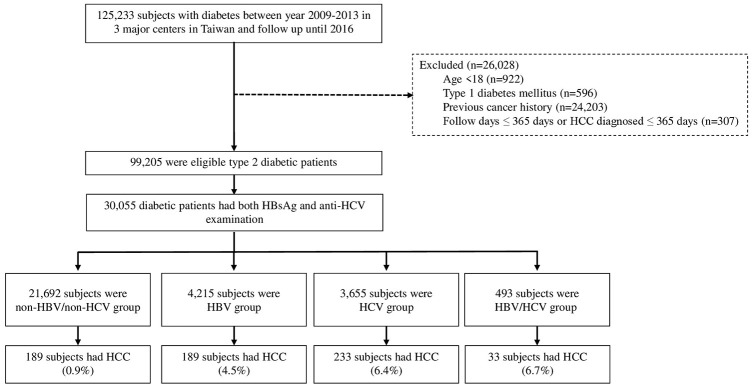
Methods: This study analyzed 30,055 individuals with T2D from the Chang Gung Research Database (2009-2016), stratified into non-HBV/non-HCV, HBV, and HCV groups. Glycemic burden was assessed using baseline glycated hemoglobin (HbA1c), high HbA1c variability, and optimal glycemic control, defined as maintaining HbA1c <7% for more than 80% of the follow-up period. Cox proportional hazard models were used to identify HCC risk factors.
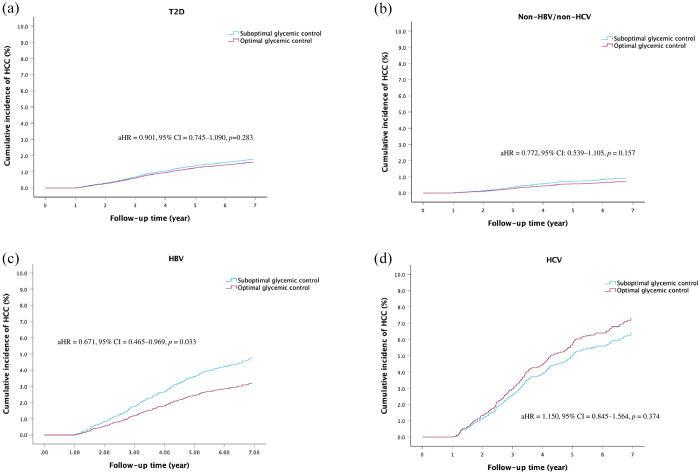
Results: Over a mean follow-up of 6.4 years, 644 individuals (2.14%) developed HCC. Viral hepatitis was the predominant independent risk factor, followed by elevated fibrosis-4 (FIB-4) scores, male sex, older age, low albumin, and low platelet count. Neither baseline HbA1c nor high HbA1c variability was associated with HCC risk in the overall T2D population or stratified groups. However, optimal glycemic control was significantly associated with reduced HCC risk in individuals with HBV (adjusted hazard ratio (HR) = 0.671, 95% confidence interval (CI) = 0.465-0.969, p = 0.033) and demonstrated a potentially beneficial role in non-HBV/non-HCV patients with presumed metabolic dysfunction-associated fatty liver disease (presumed MAFLD; adjusted HR = 0.574, 95% CI: 0.309-1.065, p = 0.079).
Conclusion: Optimal glycemic control may reduce HCC risk in individuals with T2D and HBV and potentially benefits those with presumed MAFLD, although its role in HCV-related HCC appears limited. These findings highlight the need for tailored glycemic management strategies based on viral hepatitis type.
Keywords: glycemic control; hepatitis B; hepatitis C; hepatocellular carcinoma; type 2 diabetes.
Plain language summary
How does blood sugar control impact liver cancer risk in people with type 2 diabetes and hepatitis infections? Liver cancer, specifically hepatocellular carcinoma (HCC), is a leading cause of cancer-related deaths worldwide. People with type 2 diabetes have a higher risk of developing HCC. This study explored how blood sugar control (glycemic control) affects HCC risk in people with type 2 diabetes and chronic hepatitis B or C infections. Why did we conduct this research? Chronic hepatitis B (HBV) and hepatitis C (HCV) are major causes of liver cancer. Type 2 diabetes further increases HCC risk. However, it is unclear whether controlling blood sugar can reduce this risk in people with hepatitis. This study aimed to find out if better glycemic control lowers HCC risk in individuals with type 2 diabetes and hepatitis. How did we conduct the study? We analyzed health records from over 30,000 people with type 2 diabetes in Taiwan. Participants were divided into four groups based on their hepatitis status: no hepatitis, HBV, HCV, and both HBV/HCV. We measured blood sugar control using HbA1c levels, defining good control as keeping HbA1c below 7% for at least 80% of the follow-up period. What did we find? Viral hepatitis was the strongest risk factor for HCC. Glycemic control had different effects based on hepatitis status: HBV: Good blood sugar control reduced HCC risk by 33%. HCV: Blood sugar control did not significantly lower HCC risk. No Hepatitis: There was a trend suggesting a lower HCC risk, especially in people with presumed metabolic dysfunction-associated fatty liver disease (presumed MAFLD) Conclusion: Maintaining good blood sugar control can reduce liver cancer risk in people with type 2 diabetes, particularly those with HBV infection. More research is needed to understand why glycemic control has limited benefits for those with HCV.
© The Author(s), 2025.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures



Similar articles
-
Pharmacological interventions for acute hepatitis C infection: an attempted network meta-analysis.Cochrane Database Syst Rev. 2017 Mar 13;3(3):CD011644. doi: 10.1002/14651858.CD011644.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2018 Dec 03;12:CD011644. doi: 10.1002/14651858.CD011644.pub3. PMID: 28285495 Free PMC article. Updated.
-
Direct-acting antivirals for chronic hepatitis C.Cochrane Database Syst Rev. 2017 Sep 18;9(9):CD012143. doi: 10.1002/14651858.CD012143.pub3. Cochrane Database Syst Rev. 2017. PMID: 28922704 Free PMC article.
-
Pharmacological interventions for acute hepatitis B infection: an attempted network meta-analysis.Cochrane Database Syst Rev. 2017 Mar 21;3(3):CD011645. doi: 10.1002/14651858.CD011645.pub2. Cochrane Database Syst Rev. 2017. PMID: 28321877 Free PMC article.
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.Health Technol Assess. 2006 Aug;10(28):iii-iv, xi-xiv, 1-183. doi: 10.3310/hta10280. Health Technol Assess. 2006. PMID: 16904047
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
References
-
- Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers 2021; 7: 6. - PubMed
-
- Villanueva A. Hepatocellular carcinoma. N Engl J Med 2019; 380: 1450–1462. - PubMed
-
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2024; 74: 229–263. - PubMed
-
- El-Serag HB. Hepatocellular carcinoma. N Engl J Med 2011; 365: 1118–1127. - PubMed
LinkOut - more resources
Full Text Sources
