

Interventions to Reduce the Risk of Hypocalcemia After Parathyroidectomy for People With Advanced Chronic Kidney Disease: A Systematic Review
- PMID: 40756446
- PMCID: PMC12314243
- DOI: 10.1177/20543581251358144
Interventions to Reduce the Risk of Hypocalcemia After Parathyroidectomy for People With Advanced Chronic Kidney Disease: A Systematic Review
Abstract
Background: People with advanced chronic kidney disease (CKD) and secondary hyperparathyroidism (sHPT) refractory to medical therapy often require surgical parathyroidectomy. Severe and prolonged hypocalcemia immediately following parathyroidectomy for sHPT is often termed "hungry bone syndrome" (HBS).
Objective: To systematically review the effect of pre-operative interventions on post-operative hypocalcemia, HBS, and other related outcomes in patients with CKD and sHPT undergoing parathyroidectomy.
Design: This is a systematic review study.
Setting: Diverse study designs conducted in any country.
Patients: Adult patients with CKD complicated by sHPT undergoing parathyroidectomy.
Measurements: Post-operative hypocalcemia, HBS, symptomatic hypocalcemia, and other related outcomes.
Methods: We searched Ovid MEDLINE, Embase, and Cochrane Controlled Trials Registry from inception until June 2024 for trials and observational studies of adults with CKD and sHPT that evaluated pre-operative interventions aimed at reducing the risk of hypocalcemia following parathyroidectomy. After 2 phases of study screening conducted in duplicate, we extracted data on study design, patient characteristics, interventions, and outcomes. Hypocalcemia was defined as serum calcium <2.1 mmol/L and HBS as calcium <2.1 mmol/L for ≥4 days post-operatively. We evaluated the risk of bias and completed a narrative synthesis of the available literature across intervention types.
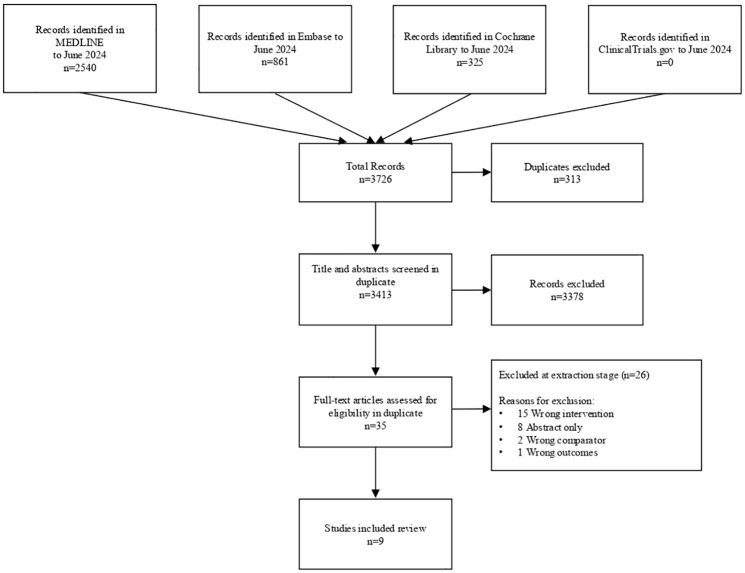
Results: We identified 3616 studies; 35 underwent full-text review, and 9 met final eligibility criteria. Interventions included pre-operative calcitriol (n = 2), pre-operative cinacalcet (n = 3), pre-operative alkaline phosphatase (ALP) measurement to guide intravenous (IV) calcium administration (n = 3), and pre-operative pamidronate (n = 1). All studies reported on at least one of: median/mean post-operative calcium (n = 7), incidence of post-operative hypocalcemia (n = 3), HBS (n = 1), and symptomatic hypocalcemia (n = 4). Interventions that reported on the risk of post-operative hypocalcemia included pre-operative pamidronate (n = 1, 37 participants, odds ratio [OR] = 0.003, 95% confidence interval [CI] = 0.000-0.072) and IV calcium guided by pre-operative ALP (n = 1, 271 participants, OR = 0.292, 95% CI = 0.175-0.488). There were insufficient data to meta-analyze study-specific effects for any intervention or outcome.
Limitations: Our study was limited by significant heterogeneity in outcome reporting, which resulted in substantial outcome reporting bias and prevented pooled analyses. Furthermore, no randomized control trials met our inclusion criteria, which limited assessment of publication bias.
Conclusions: Pre-operative risk factors for HBS have been established in patients with CKD undergoing parathyroidectomy. However, limited research has evaluated pre-operative interventions to reduce the risk of HBS, and due to heterogeneity in outcome reporting across studies, there is still uncertainty about the effectiveness of such interventions. These findings support the need for future clinical trials.
Contexte: Il est fréquent que les personnes atteintes d’insuffisance rénale chronique (IRC) de stade avancé qui souffrent d’hyperparathyroïdie secondaire (HPTs) réfractaire au traitement médical aient besoin d’une parathyroïdectomie. L’hypocalcémie grave et prolongée qui survient immédiatement après cette intervention est souvent désignée sous le terme « hungry bone syndrome » (HBS) ou « hypocalcémie par avidité osseuse ».
Objectif: Procéder à un examen systématique de l’effet de certaines interventions préopératoires sur l’hypocalcémie postopératoire, l’HBS et d’autres issues cliniques associés chez les patients atteints d’IRC et d’HPTs subissant une parathyroïdectomie.
Conception: Revue systématique.
Cadre: Divers modèles d’études, sans égard au pays de l’étude.
Sujets: Les adultes atteints d’IRC compliquée par une HPTs qui ont subi une parathyroïdectomie.
Mesures: Hypocalcémie post-opératoire, HBS, hypocalcémie symptomatique et autres issues cliniques associés à la parathyroïdectomie.
Méthodologie: Nous avons consulté les bases de données Ovid MEDLINE et Embase, ainsi que le registre central Cochrane des essais contrôlés, depuis leur création jusqu’en juin 2024, à la recherche d’essais et d’études observationnelles portant sur des adultes atteints d’IRC et d’HPTs, et évaluant des interventions préopératoires visant à réduire le risque d’hypocalcémie après une parathyroïdectomie. Après une revue de littérature effectuée en deux phases et de façon indépendante par deux auteurs, nous avons extrait des données sur la conception de l’étude, les caractéristiques des patients, les interventions et les issues cliniques. L’hypocalcémie a été définie par une calcémie inférieure à 2,1 mmol/l et l’HBS par une calcémie inférieure à 2,1 mmol/l persistant au moins 4 jours après la chirurgie. Nous avons évalué les risques de biais et procédé à une synthèse narrative de la documentation disponible pour tous les types d’interventions.
Résultats: Des 3 616 études identifiées, 35 ont fait l’objet d’un examen du texte intégral et, en définitive, 9 études répondaient aux critères d’admissibilité. Les interventions préopératoires examinées comprenaient l’administration de calcitriol (n=2 études), l’administration de cinacalcet (n=3 études), la mesure de la phosphatase alcaline (PAL) pour guider l’administration intraveineuse (IV) de calcium (n=3 études) et l’administration de pamidronate (n=1 étude). Toutes les études rapportaient au moins une des données suivantes: calcium médian/moyen postopératoire (n=7 études), incidence de l’hypocalcémie postopératoire (n=3 études), HBS (n=1 étude) et hypocalcémie symptomatique (n=4 études). Les interventions réalisées dans les études ayant examiné le risque d’hypocalcémie postopératoire étaient l’administration de pamidronate préopératoire (1 étude; 37 participants; OR 0,003; IC à 95 %: 0,000-0,072) et l’administration de calcium IV guidée par une mesure préopératoire de la PAL (1 étude; 271 participants; OR 0,292; IC à 95 %: 0,175-0,488). Les données étaient insuffisantes pour permettre une méta-analyse des effets spécifiques à l’étude pour tout évènement clinique ou intervention.
Limites: L’importante hétérogénéité dans la présentation des résultats a entraîné un biais important et empêché les analyses groupées. Aucun essai contrôlé randomisé ne répondait aux critères d’inclusion, ce qui a limité l’évaluation du biais de publication.
Conclusion: Des facteurs de risque préopératoires pour l’HBS ont été établis chez les patients atteints d’IRC qui subissent une parathyroïdectomie. Cependant, peu d’études ont évalué les interventions préopératoires visant à réduire le risque d’HBS, et en raison de l’importante hétérogénéité entre les études dans la présentation des résultats, une incertitude persiste quant à l’efficacité de ces interventions. Nos résultats confirment que d’autres essais cliniques sont nécessaires.
Keywords: chronic kidney disease; hungry bone syndrome; hypocalcemia; parathyroidectomy; secondary hyperparathyroidism.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Similar articles
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Conservative, physical and surgical interventions for managing faecal incontinence and constipation in adults with central neurological diseases.Cochrane Database Syst Rev. 2024 Oct 29;10(10):CD002115. doi: 10.1002/14651858.CD002115.pub6. Cochrane Database Syst Rev. 2024. PMID: 39470206
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2020 Jan 9;1(1):CD011535. doi: 10.1002/14651858.CD011535.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 19;4:CD011535. doi: 10.1002/14651858.CD011535.pub4. PMID: 31917873 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Tsai WC, Peng YS, Yang JY, et al. Short- and long-term impact of subtotal parathyroidectomy on the achievement of bone and mineral parameters recommended by clinical practice guidelines in dialysis patients: a 12-year single-center experience. Blood Purif. 2013;36(2):116-121. doi: 10.1159/000353415. - DOI - PubMed
-
- Mittendorf EA, Merlino JI, McHenry CR. Post-parathyroidectomy hypocalcemia: incidence, risk factors, and management. Am Surg. 2004;70(2):114-119. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
