

Subxiphoid Thoracoscopic Surgery Is Safe and Feasible for the Treatment of Anterior Mediastinal Teratomas: A Multicentre Retrospective Study
- PMID: 40758465
- PMCID: PMC12343096
- DOI: 10.1093/ejcts/ezaf267
Subxiphoid Thoracoscopic Surgery Is Safe and Feasible for the Treatment of Anterior Mediastinal Teratomas: A Multicentre Retrospective Study
Abstract
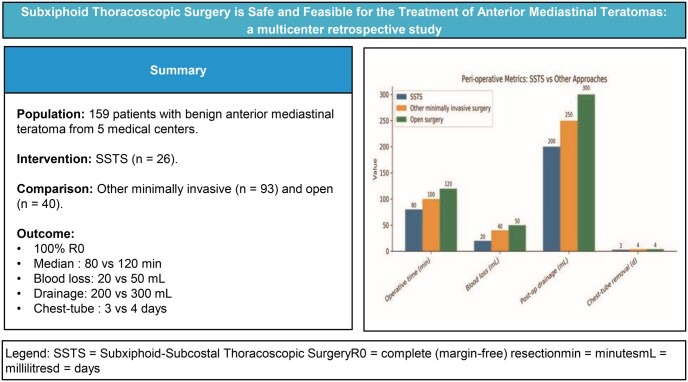
Background: Mediastinal benign teratoma is rare, with surgery being the only effective treatment. Few studies reported the surgical outcomes of resecting mediastinal benign teratomas via the subxiphoid approach by thoracoscopy. This study retrospectively compares the subxiphoid with other surgical approaches, aiming to assess the safety and feasibility of this technique.
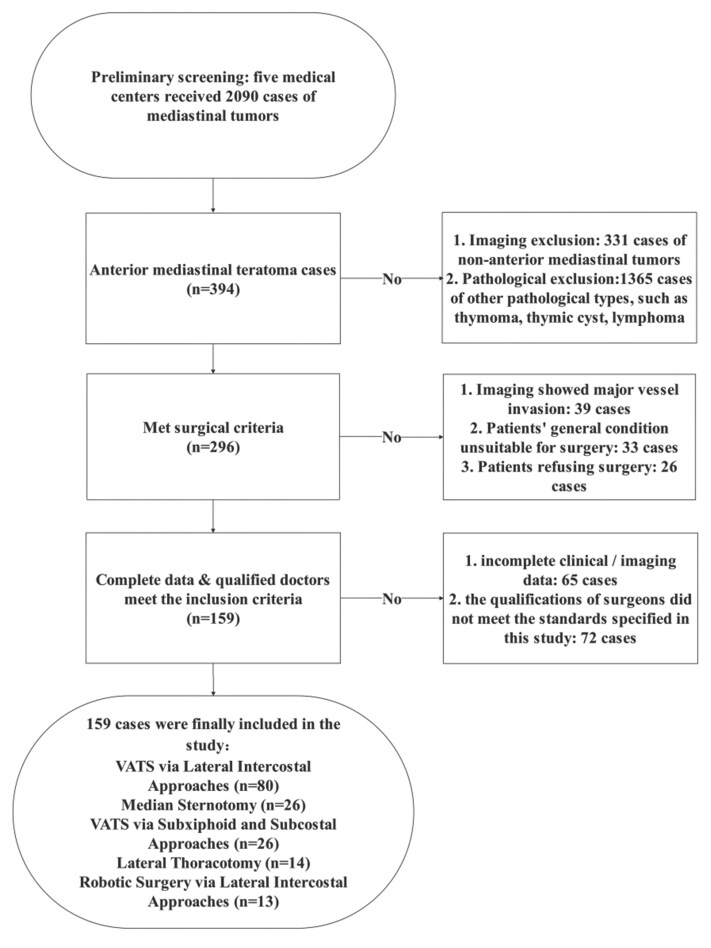
Methods: We retrospectively analysed the clinical data of 159 patients with pathologically confirmed mediastinal benign teratomas who underwent surgery in 5 hospitals from July 2014 to June 2024. Various parameters of the subxiphoid approach were compared with those of other surgical methods.
Results: The surgical approaches included median sternotomy in 26 cases, lateral thoracotomy in 14 cases, lateral thoracoscopic surgery in 80 cases, subxiphoid thoracoscopic surgery in 26 cases, and robotic surgery in 13 cases. For patients who underwent the subxiphoid approach, the median surgery time was 80 min (70, 90), the median intraoperative blood loss was 20 mL (10, 20), the median postoperative drainage volume was 200 mL (0, 350), and the median time to drain removal was 3 days (0, 3). Complete tumour resection was achieved in all 26 patients (100%). The subxiphoid approach showed advantages in the aforementioned aspects compared to other surgical methods.
Conclusions: The subxiphoid and subcostal arch approach is a safe and feasible surgical technique for benign anterior mediastinal teratoma, with a potentially faster postoperative recovery and less cost. It is a valuable alternative to conventional median sternotomy, lateral thoracotomy, and lateral thoracoscopic surgery in resection of anterior mediastinal teratoma.
Keywords: anterior mediastinal tumour; subxiphoid; teratoma; thoracoscopic surgery.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Conflict of interest statement
J.G., Y.L., E.X., F.K., G.H., S.H., C.Lia., Y.L., C.Li., L.S., Y.P., and H.R. have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Takeda S, Miyoshi S, Ohta M, Minami M, Masaoka A, Matsuda H. Primary germ cell tumors in the mediastinum: a 50-year experience at a single Japanese institution. Cancer. 2003;97:367-376. - PubMed
-
- Dulmet EM, Macchiarini P, Suc B, Verley JM. Germ cell tumors of the mediastinum. A 30-year experience. Cancer. 1993;72:1894-1901. - PubMed
-
- Moran CA, Suster S. Primary germ cell tumors of the mediastinum: I. Analysis of 322 cases with special emphasis on teratomatous lesions and a proposal for histopathologic classification and clinical staging. Cancer. 1997;80:681-690. - PubMed
-
- Chang CC, Chang YL, Lee JM, et al. 18 Years surgical experience with mediastinal mature teratoma. J Formos Med Assoc. 2010;109:287-292. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
