

Personalized colorectal cancer risk assessment through explainable AI and Gut microbiome profiling
- PMID: 40760681
- PMCID: PMC12326576
- DOI: 10.1080/19490976.2025.2543124
Personalized colorectal cancer risk assessment through explainable AI and Gut microbiome profiling
Abstract
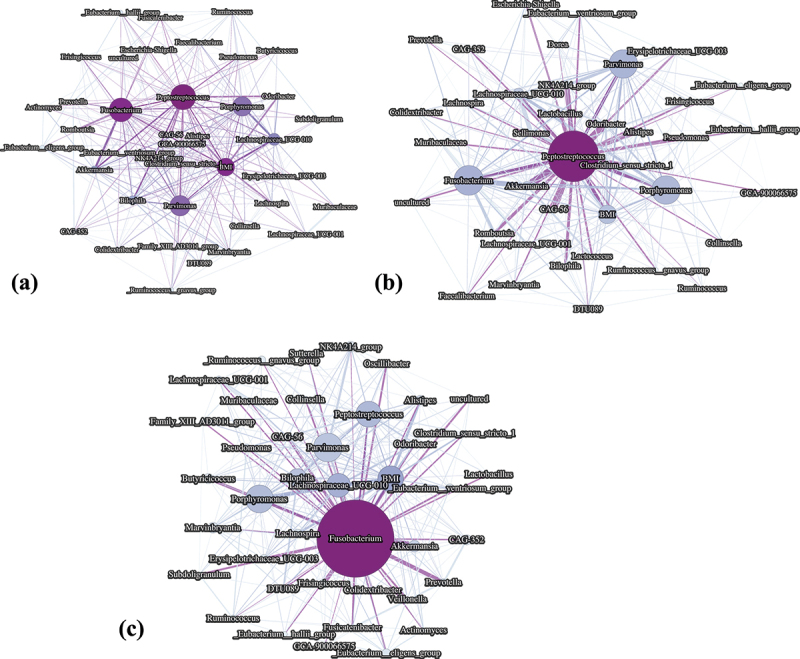
The clinical adenoma - carcinoma progression represents a well-established framework for understanding colorectal cancer (CRC) development, although the molecular mechanisms underlying this transition remain only partially understood. Increasing evidence suggests the gut microbiome (GM) as a key modulator of colorectal carcinogenesis, positioning microbial profiling as a promising avenue for noninvasive risk stratification and early detection. In this study, Machine Learning (ML) classifiers integrated with eXplainable Artificial Intelligence (XAI) techniques were employed to identify microbiome-derived biomarkers predictive of CRC and adenomatous lesions. The models were trained on 16S rRNA sequencing data from 453 patients and evaluated through cross-validation, achieving AU-ROC and AU-PRC scores of 0.71 and 0.67, respectively. External validation on an independent Italian cohort () yielded AU-ROC and AU-PRC scores of 0.70 and 0.89, respectively. XAI-based interpretation revealed consistent microbial signatures across datasets. In detail, taxa belonging to the Fusobacterium and Peptostreptococcus genera were associated with increased CRC risk, whereas the Eubacterium eligens group was identified as a robust negative predictor. Beyond classification, patient-level explanations enabled by XAI facilitated the identification of adenoma subgroups exhibiting microbiome profiles converging toward those of CRC, suggesting the presence of transitional microbial states. Moreover, SHAP-based interaction networks uncovered microbial hubs and inter-species dependencies characterizing high-risk configurations, providing insights into the ecological dynamics of colorectal tumorigenesis. These findings demonstrate the added XAI value in elucidating microbiome interactions, enhancing model interpretability, and supporting biologically informed hypotheses. This integrative, explainable framework highlights the potential of AI-driven microbiome analysis in precision oncology and advances the development of interpretable, noninvasive tools for CRC risk prediction and management.
Keywords: Explainable AI; SHAP interaction analysis; biomarker; colorectal cancer; microbiome; risk stratification.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures






References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical