

Visualizations of autoregulatory insults in moderate-to-severe paediatric traumatic brain injury: a secondary analysis from the multicentre STARSHIP trial
- PMID: 40760697
- PMCID: PMC12323160
- DOI: 10.1186/s13054-025-05568-4
Visualizations of autoregulatory insults in moderate-to-severe paediatric traumatic brain injury: a secondary analysis from the multicentre STARSHIP trial
Abstract
Background: Paediatric traumatic brain injury (TBI) is a heterogeneous condition with age-dependent differences in systemic and cerebral physiology, making cerebral perfusion pressure (CPP) challenging to target. Monitoring cerebral autoregulation using the pressure reactivity index (PRx) and deriving an autoregulatory optimal CPP (CPPopt) may personalize treatment, but evidence in children remains limited. In this multicentre paediatric TBI study, we aimed to explore and visualize PRx and CPPopt in relation to outcome.
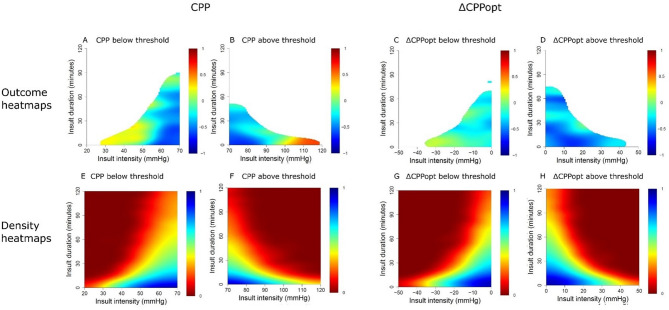
Methods: In this secondary analysis of the prospective, multicentre study (STARSHIP), 98 paediatric TBI patients (1-16 years) from 10 paediatric intensive care units, in the UK, between 2018 and 2023, with high-frequency physiological data and 12-month GOS-E Peds outcomes, not treated with decompressive craniectomy, were included. Intracranial pressure (ICP), PRx, CPP, and ΔCPPopt were correlated with outcome using insult intensity/duration heatmaps across the full monitoring period. Two-variable heatmaps incorporating PRx were also used to assess how autoregulation modified the relationship between ICP, CPP, and ΔCPPopt with outcome.
Results: There was a transition from favourable to unfavourable outcome when PRx exceeded + 0.00 for longer episodes. Furthermore, there was a transition towards worse outcome when CPP went below 40 mmHg and above 100 mmHg for sustained durations. For ΔCPPopt, the transition towards poor prognosis occurred for values below - 20 mmHg, but positive ΔCPPopt was tolerated. In the two-variable heatmaps, PRx above + 0.50 together with ICP above 20 mmHg, CPP below 60 mmHg, or negative ΔCPPopt were particularly associated with unfavourable outcome.
Conclusions: This novel study visualized the safe and dangerous intervals for PRx and CPPopt as well as the interaction effect between the autoregulatory status and ICP, CPP, and ΔCPPopt in relation to outcome in paediatric TBI. Future prospective trials are needed to evaluate the safety, feasibility, and efficacy of PRx/CPPopt guided management.
Keywords: Cerebral autoregulation; Optimal cerebral perfusion pressure; Outcome; Paediatric; Pressure reactivity index; Traumatic brain injury.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Health Research Authority, South West-Central Bristol Research Ethics Committee (Ref: 18/SW/0053, 23/SW/011). Informed consent was obtained by the patients’ caregivers. Consent for publication: Not applicable. Competing interests: ICM+ is a software licensed by Cambridge Enterprise Ltd. PS has a financial interest in a part of licensing fee; the licensing fee was waivered for this study.
Figures


References
-
- Hawley CA, Ward AB, Long J, Owen DW, Magnay AR. Prevalence of traumatic brain injury amongst children admitted to hospital in one health district: a population-based study. Injury. 2003;34(4):256–60. - PubMed
-
- Wooldridge G, Hansmann A, Aziz O, O’Brien N. Survey of resources available to implement severe pediatric traumatic brain injury management guidelines in low and middle-income countries. Childs Nerv Syst. 2020;36(11):2647–55. - PubMed
-
- Liang KWH, Lee JH, Qadri SK, Nadarajan J, Caporal P, Roa GJ, González-Dambrauskas S, Abbas Q, Kazzaz Y, Chong SL. Differences in clinical outcomes and resource utilization in pediatric traumatic brain injury between countries of different sociodemographic indices. J Neurosurg Pediatr. 2024;33(5):461–8. - PubMed
-
- Kochanek PM, Tasker RC, Carney N, Totten AM, Adelson PD, Selden NR, Davis-O’Reilly C, Hart EL, Bell MJ, Bratton SL, et al. Guidelines for the management of pediatric severe traumatic brain injury, third edition: update of the brain trauma foundation guidelines. Pediatr Crit Care Med. 2019;20(3S Suppl 1):S1–82. - PubMed
-
- Mehta A, Kochanek PM, Tyler-Kabara E, Adelson PD, Wisniewski SR, Berger RP, Sidoni MD, Bell RL, Clark RS, Bell MJ. Relationship of intracranial pressure and cerebral perfusion pressure with outcome in young children after severe traumatic brain injury. Dev Neurosci. 2010;32(5–6):413–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
