

The relationship between clinical subtypes, prognosis, and treatment in ICU patients with acute cholangitis using unsupervised machine learning methods
- PMID: 40760727
- PMCID: PMC12323092
- DOI: 10.1186/s12879-025-11346-y
The relationship between clinical subtypes, prognosis, and treatment in ICU patients with acute cholangitis using unsupervised machine learning methods
Abstract
Background: Acute cholangitis (AC) presents with significant clinical heterogeneity, and existing severity classifications have limited prognostic value in critically ill patients. Subtypes of AC in critically ill patients have not been investigated.
Objective: The study aimed to offer a novel approach to identify clinical subtypes and improve individualized risk assessment and treatment strategies using an unsupervised analysis.
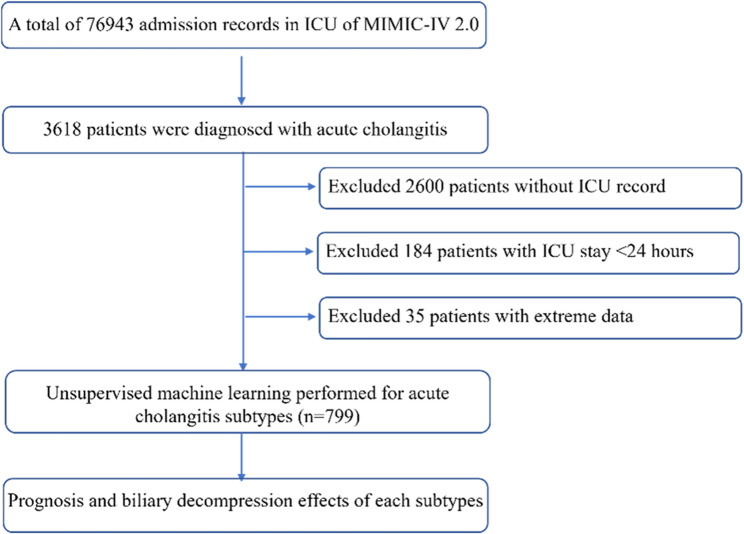
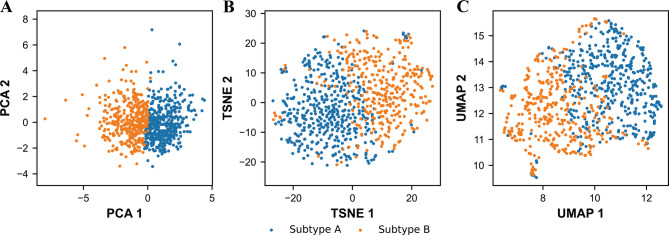
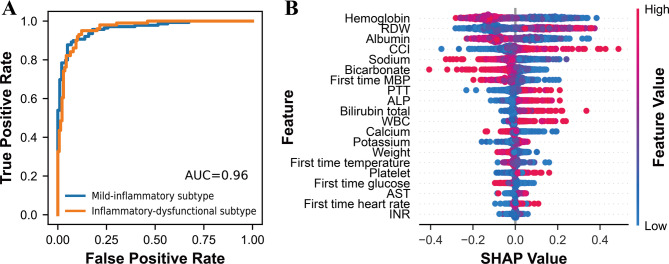
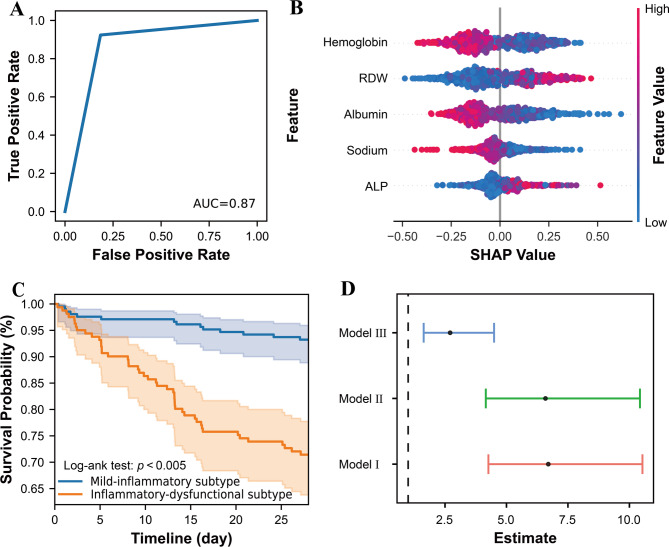
Methods: We conducted a retrospective analysis of ICU patients with AC from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database. K-means clustering was applied to 24 routinely available clinical variables from the first 24 h of ICU admission to identify clinical subtypes. The primary outcome was 28-day all-cause mortality. Multivariable Cox regression was used to assess associations between subtypes, mortality, and biliary drainage strategies. Furthermore, a simplified model using the top five SHapley Additive exPlanations (SHAP) ranked variables (hemoglobin, RDW, albumin, CCI, and sodium) was developed and subsequently validated in an external cohort from MIMIC-III.
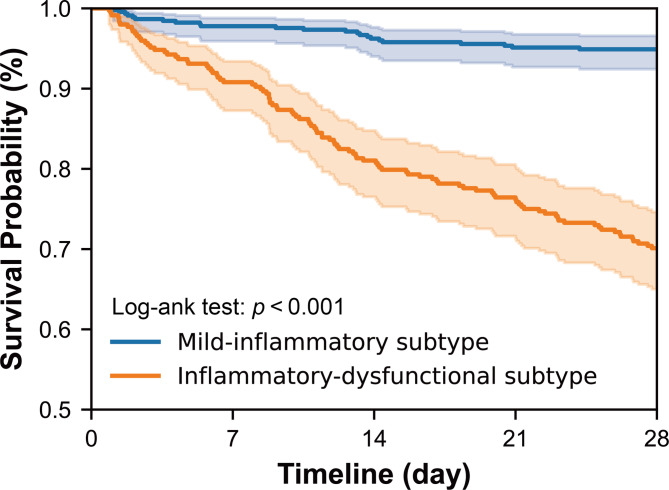
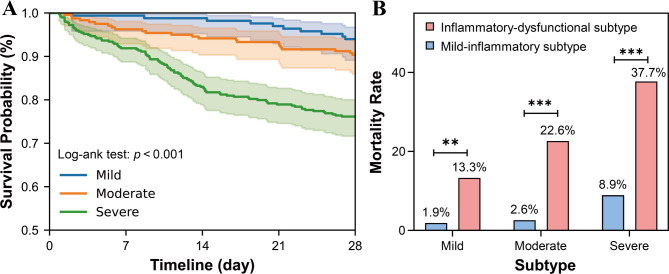
Results: Two distinct subtypes were identified: a mild-inflammatory subtype (n = 451) and an inflammatory-dysfunctional subtype (n = 348). The inflammatory-dysfunctional subtype was characterized by higher levels of RDW, ALP, bilirubin, creatinine, and coagulopathy markers, and exhibited significantly higher 28-day mortality (30.17% vs. 5.32%, p < 0.001). This subtype remained an independent predictor of mortality after multivariable adjustment (HR = 2.38,95%CI:1.42-3.9, p = 0.001). Within the inflammatory-dysfunctional subtype, ERCP was associated with lower mortality (HR = 0.56, p = 0.01), whereas PTCD was associated with higher mortality (HR = 1.63, p = 0.031), potentially reflecting underlying disease severity. The simplified model retained strong discriminative performance (AUC = 0.87) and was successfully validated in the external cohort, confirming the reproducibility and prognostic relevance of the subtypes.
Conclusions: We identified and externally validated two clinically meaningful AC subtypes with distinct prognoses. A simplified model using five readily available variables facilitates clinical application and can support more individualized treatment approaches. These data-driven subtypes offer additional prognostic discrimination beyond the Tokyo Guidelines, serving as a valuable complement to existing severity classifications for guiding precision management of ICU patients with AC.
Keywords: Acute cholangitis; K-means clustering; Prognosis; Subtype.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in line with the principles of the Declaration of Helsinki. The MIMIC database follows a review board protocol in which all patient personal information is de-identified, using random codes to identify specific patients. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Yokoe M, Hata J, Takada T, Strasberg SM, Asbun HJ, Wakabayashi G, Kozaka K, Endo I, Deziel DJ, Miura F, Okamoto K, Hwang TL, Huang WS, Ker CG, Chen MF, Han HS, Yoon YS, Choi IS, Yoon DS, Noguchi Y, Shikata S, Ukai T, Higuchi R, Gabata T, Mori Y, Iwashita Y, Hibi T, Jagannath P, Jonas E, Liau KH, Dervenis C, Gouma DJ, Cherqui D, Belli G, Garden OJ, Gimenez ME, de Santibanes E, Suzuki K, Umezawa A, Supe AN, Pitt HA, Singh H, Chan ACW, Lau WY, Teoh AYB, Honda G, Sugioka A, Asai K, Gomi H, Itoi T, Kiriyama S, Yoshida M, Mayumi T, Matsumura N, Tokumura H, Kitano S, Hirata K, Inui K, Sumiyama Y, Yamamoto M. Tokyo guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018;25(1):41–54. - PubMed
-
- Beliaev AM, Zyul’korneeva S, Rowbotham D, Bergin CJ. Screening acute cholangitis patients for sepsis. ANZ J Surg. 2019;89(11):1457–61. - PubMed
-
- Gulumsek E, Yesildal F, Yigitdol I, Erdem I, Arbag HC, Avci A, Saler T, Kara B, Tas A, Sumbul HE. Should lactate be added to Tokyo criteria for the evaluation of patients with acute cholangitis? Ir J Med Sci. 2022;191(3):1177–83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
