

Case report: proximal tibiofibular joint instability-a forgotten cause in revision total knee arthroplasty?
- PMID: 40761198
- PMCID: PMC12319615
- DOI: 10.21037/acr-25-46
Case report: proximal tibiofibular joint instability-a forgotten cause in revision total knee arthroplasty?
Abstract
Background: Proximal tibiofibular joint instability (PTJI) is a rare condition, particularly in total knee arthroplasty (TKA) revision, with only one prior case reported. This case highlights the importance of considering PTJI in patients with chronic lateral knee pain and instability following TKA and demonstrates a novel stabilization approach for managing this challenging condition.
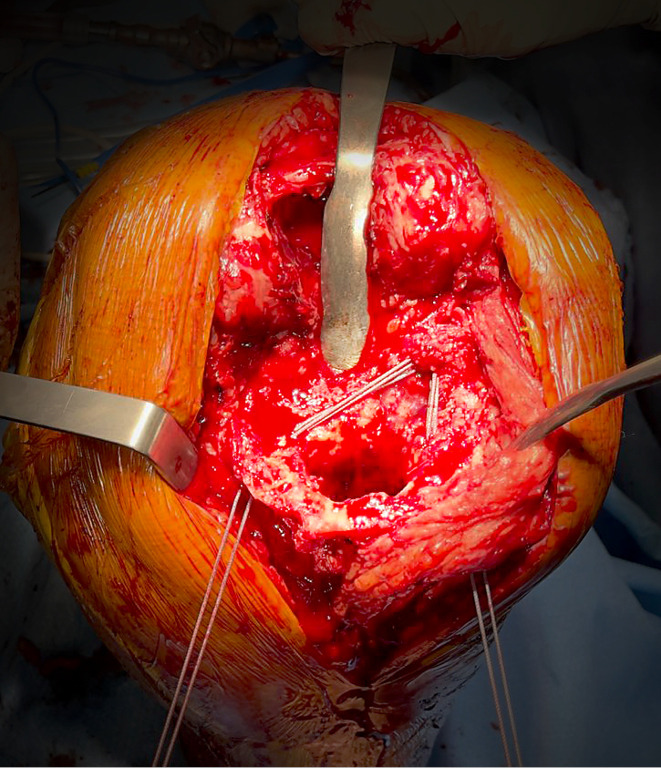
Case description: A 73-year-old female with a history of multiple knee surgeries presented to our clinic due to increasing lateral knee pain radiating along the syndesmosis, aggravated by activities like squatting. Clinical examination revealed anteroposterior subluxation of the fibular head, suggesting PTJI. Radiological findings confirmed tibial component loosening, and the diagnosis of aseptic loosening with PTJI was made. Given her complex surgical history, a two-stage revision was planned. The first stage involved prosthesis removal, bacteriological sampling, and spacer placement. The second stage included revision TKA and proximal tibiofibular joint (PTFJ) stabilization using a Twin Tail Tight-Rope™ system and Arthrex endobutton, preserving joint mobility and restoring functional stability. A hinged revision knee prosthesis was then implanted. The patient had an uneventful recovery. At 1-year follow-up, the pain score was 1/10 and she achieved good mobility. Radiographs showed satisfactory implant positioning. The Western Ontario and McMaster Universities Arthritis Index (WOMAC) score of 15/96 indicated a successful outcome.
Conclusions: PTJI is rare and is not typically associated with TKA. This case report highlights a unique presentation of PTJI in a multi-revised TKA, raising concerns about the potential role of repeated proximal tibial resections in ligamentous instability of the PTFJ. The specific localization of pain and its resolution following PTFJ fixation support this hypothesis. Therefore, careful assessment of the PTFJ should be considered in TKA revisions, particularly in cases involving extensive lateral tibial resections.
Keywords: Proximal tibiofibular joint instability (PTJI); case report; complications in total knee arthroplasty (complications in TKA); ligamentous injury; revision knee surgery.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://acr.amegroups.com/article/view/10.21037/acr-25-46/coif). The authors have no conflicts of interest to declare.
Figures





References
-
- Nunes J, Direito-Santos B, Costa A, et al. Acute proximal tibiofibular joint dislocation: a sports related injury?—two different cases. Ann Joint 2019;4:11.
-
- Ogden JA. Subluxation and dislocation of the proximal tibiofibular joint. J Bone Joint Surg Am 1974;56:145-54. - PubMed
-
- Ogden JA. The anatomy and function of the proximal tibiofibular joint. Clin Orthop Relat Res 1974;(101):186-91. - PubMed
-
- Dennis JB, Rutledge BA. Bilateral recurrent dislocations of the superior tibiofibular joint with peroneal-nerve palsy. J Bone Joint Surg Am 1958;40-A:1146-8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources