

Comparison of intravascular imaging, physiological assessment and angiography for coronary revascularization in acute coronary syndrome: a systematic review and network meta-analysis
- PMID: 40761230
- PMCID: PMC12319024
- DOI: 10.3389/fcvm.2025.1604050
Comparison of intravascular imaging, physiological assessment and angiography for coronary revascularization in acute coronary syndrome: a systematic review and network meta-analysis
Abstract
Background: The optimal percutaneous coronary intervention (PCI) technique to treat acute coronary syndrome (ACS) requires further investigation. This network meta-analysis evaluated the effects of physiological assessment and intravascular imaging techniques on the prevalence of adverse cardiac outcomes following PCIs.
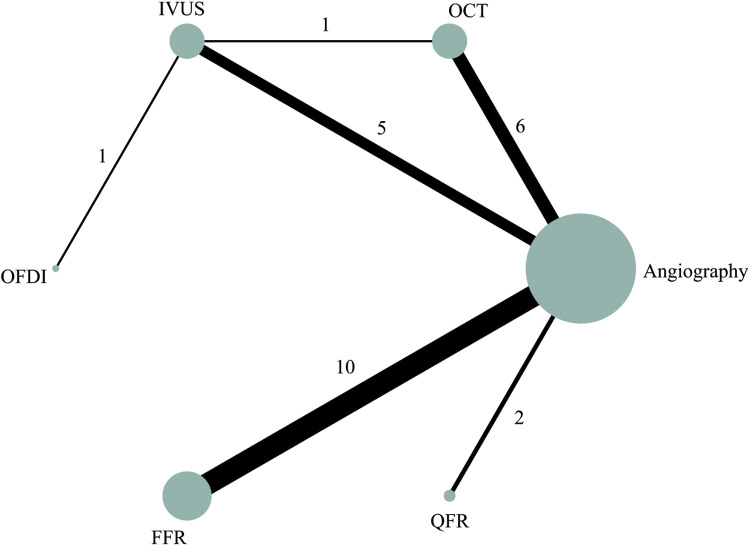
Methods: We reviewed PubMed, Cochrane, and EMBASE databases for the purpose of identifying all randomized control trials published up to October 30, 2024, comparing the impact of intravascular imaging, physiology assessment, or angiography techniques on outcomes. The primary outcome for this research was major adverse cardiovascular events (MACE) occurrences. Each PCI strategy was ranked as per the risk ratio (RR) at the 95% confidence interval (95% CI) for developing MACE.
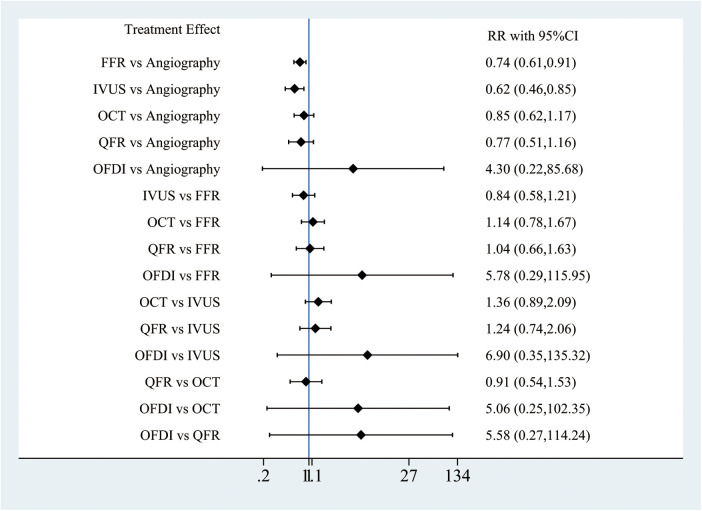
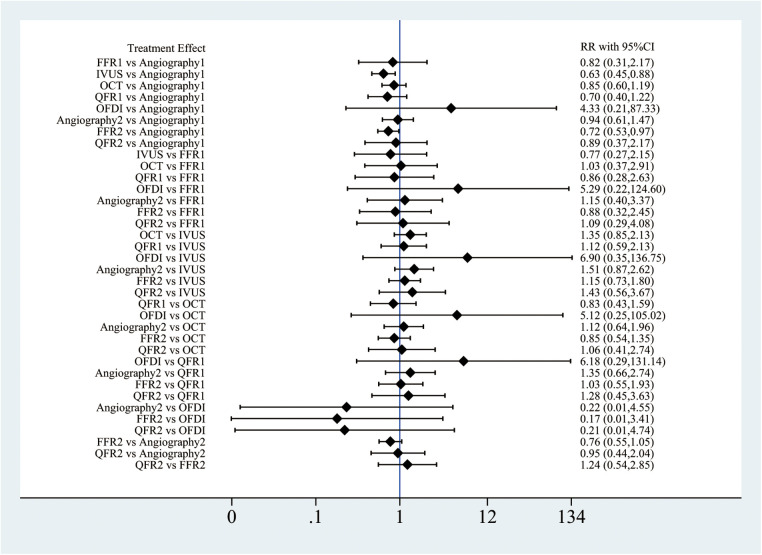
Results: Twenty-eight RCTs with 18,221 patients were identified. Compared with angiography, intravascular ultrasound (IVUS)- (RR: 0.62; 95%CI: 0.46-0.85) and fractional flow reserve (FFR)-guided PCI (RR: 0.62; 95%CI: 0.46-0.85) reduced the risk of MACE. Patients who received quantitative flow ratio (QFR)-guided PCI experienced lower all-cause mortality (RR: 0.25; 95%CI: 0.07-0.92) vs. those receiving angiography. Similarly, the RR decreased to 0.64 after using FFR-guided PCI vs. angiographic procedures (95% CI: 0.44-0.91). Compared to angiography, the subgroup analysis showed inconsistent results for IVUS-guided PCI in preventing MACE for both the optimization (RR: 0.60; 95%CI: 0.49-0.74) and decision-making (RR: 0.55; 95%CI: 0.05-6.18). The likelihood of developing MACE was lower for FFR-guided CR than for angiography-guide culprit-only PCIs (RR-0.72; 95%CI: 0.53-0.97), as confirmed by sensitivity assessment results. The research unveiled no statistically significant differences between FFR-guided culprit-only PCIs and culprit-only PCIs or angiography-guided CR.
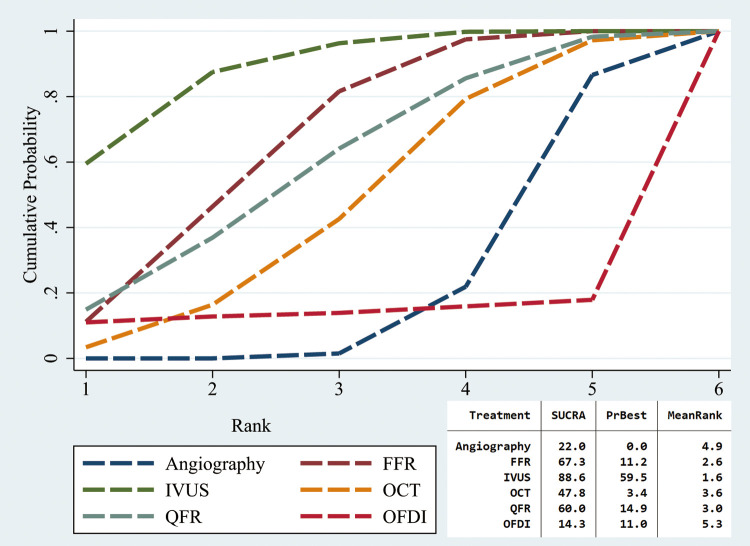
Conclusion: IVUS- and FFR-guided PCI lowers the MACE risk in patients with ACS. In addition, IVUS achieved the best results in ACS patients undergoing PCI.
Systematic review registration: INPLASY (inplasy.com), INPLASY202420092.
Keywords: acute coronary syndrome; angiography; coronary revascularization; intravascular imaging; physiology assessment.
© 2025 Liu, Ye, Wu, Lin, Lin, Li and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Intravascular ultrasound-guided versus coronary angiography-guided percutaneous coronary intervention in patients with acute myocardial infarction: A systematic review and meta-analysis.Int J Cardiol. 2022 Apr 15;353:35-42. doi: 10.1016/j.ijcard.2022.01.021. Epub 2022 Jan 15. Int J Cardiol. 2022. PMID: 35041893
-
Assessment of Coronary Stenoses for Percutaneous Coronary Intervention: A Systematic Review and Network Meta-Analysis of Randomized Trials.Am J Cardiol. 2024 Jul 15;223:29-39. doi: 10.1016/j.amjcard.2024.05.019. Epub 2024 May 18. Am J Cardiol. 2024. PMID: 38768846
-
Comparison of Intravascular Imaging, Functional, or Angiographically Guided Coronary Intervention.J Am Coll Cardiol. 2023 Dec 5;82(23):2167-2176. doi: 10.1016/j.jacc.2023.09.823. Epub 2023 Oct 23. J Am Coll Cardiol. 2023. PMID: 37995152
-
Angiography versus FFR guided complete revascularization versus culprit-only revascularization for patients presenting with STEMI: Network meta-analysis.Catheter Cardiovasc Interv. 2022 Sep;100(3):340-350. doi: 10.1002/ccd.30304. Epub 2022 Jul 5. Catheter Cardiovasc Interv. 2022. PMID: 35789058
-
Fractional Flow Reserve Directed Percutaneous Coronary Intervention Optimization Using High-Definition Intravascular Ultrasound in Non-ST-Segment Elevation Acute Coronary Syndrome Versus Chronic Coronary Syndrome.Catheter Cardiovasc Interv. 2025 Jul;106(1):12-22. doi: 10.1002/ccd.31357. Epub 2024 Dec 25. Catheter Cardiovasc Interv. 2025. PMID: 39722557 Free PMC article. Clinical Trial.
References
-
- Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J Acute Cardiovasc Care. (2024) 13(1):55–161. 10.1093/ehjacc/zuad107 Erratum in: Eur Heart J Acute Cardiovasc Care. 2024 May 28;13(5):455. doi: 10.1093/ehjacc/zuad156. - DOI - PubMed
-
- Shin DH, Hong SJ, Mintz GS, Kim JS, Kim BK, Ko YG, et al. Effects of intravascular ultrasound-guided versus angiography-guided new-generation drug-eluting stent implantation: meta-analysis with individual patient-level data from 2,345 randomized patients. JACC Cardiovasc Interv. (2016) 9(21):2232–9. 10.1016/j.jcin.2016.07.021 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous