

Weight-bearing CT as an approach to assess femoral-acetabular displacement during external rotation stress in the hip
- PMID: 40761572
- PMCID: PMC12318925
- DOI: 10.1093/jhps/hnaf001
Weight-bearing CT as an approach to assess femoral-acetabular displacement during external rotation stress in the hip
Abstract
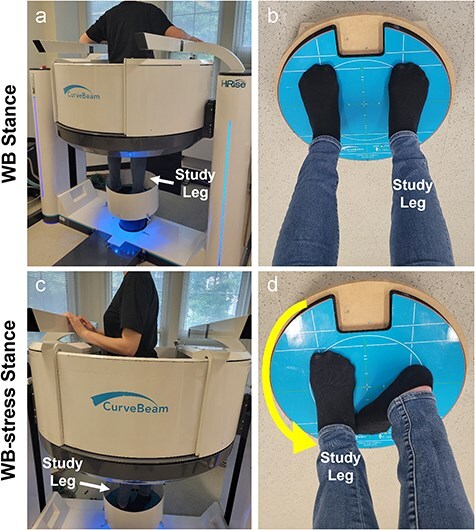
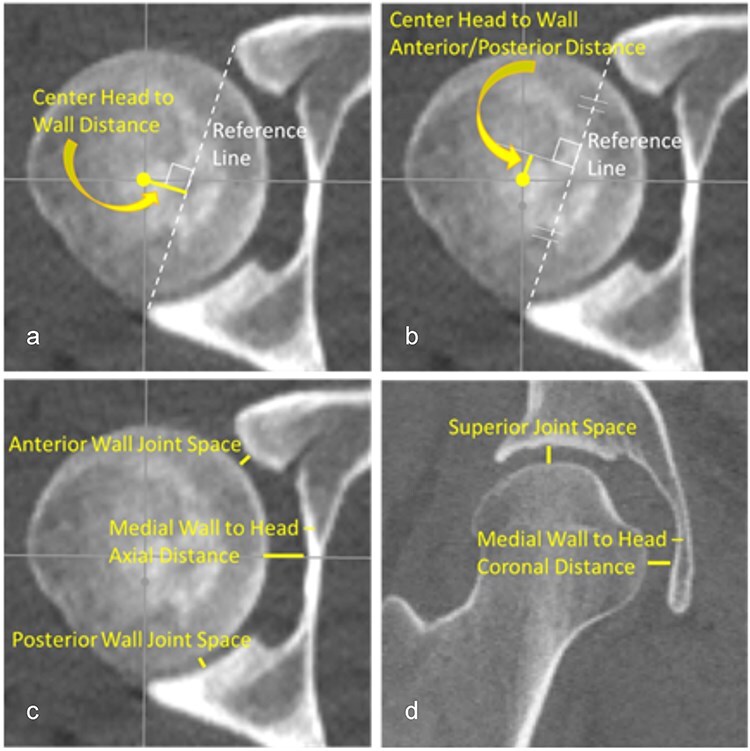
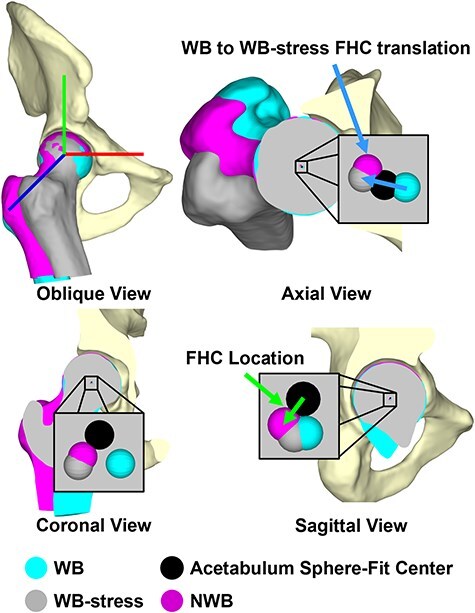
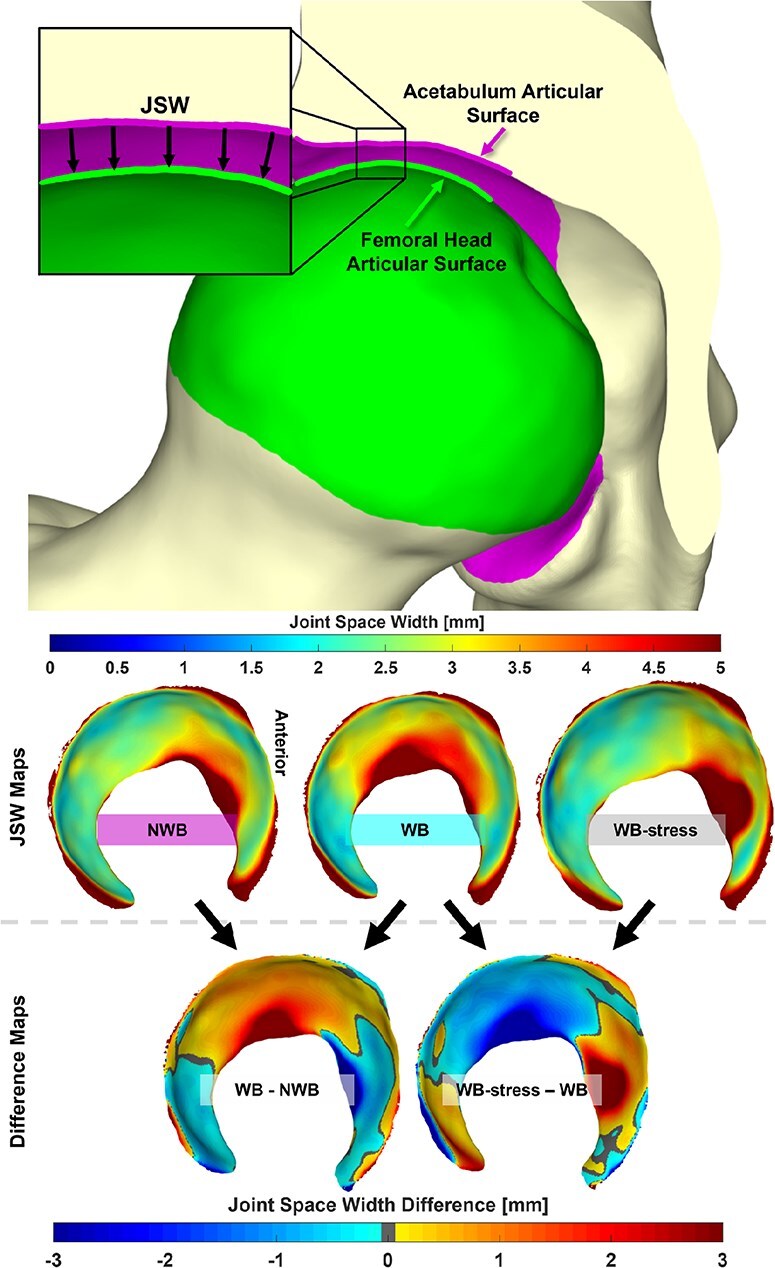
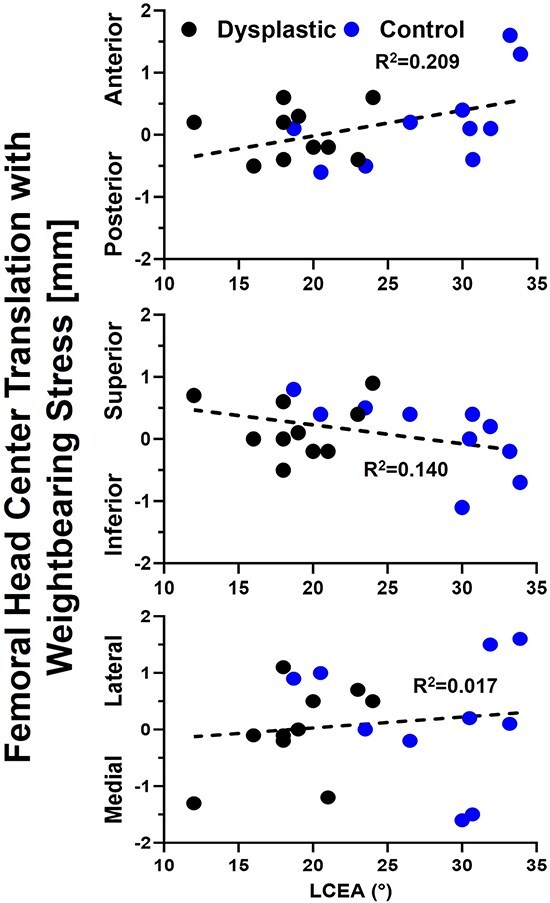
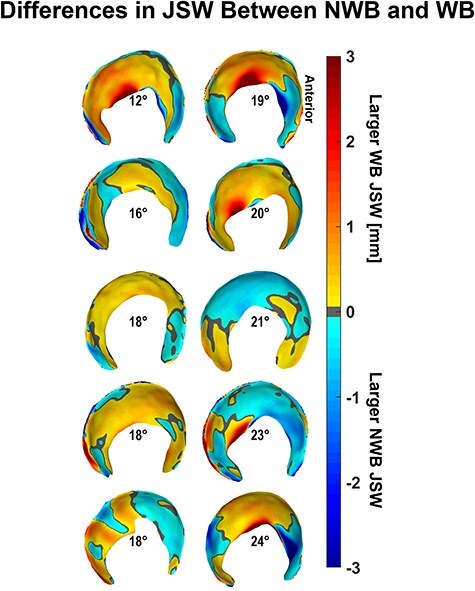
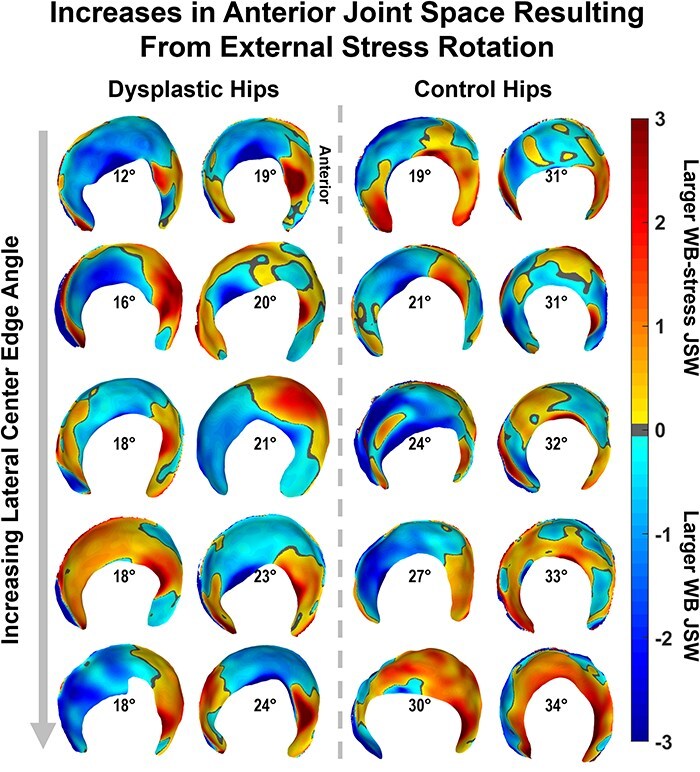
Hip dysplasia causes pathologic joint mechanics and can produce hip instability, leading to progressive joint degeneration and osteoarthritis. Weight-bearing computed tomography (WBCT) is an emerging technology that may enable quantification of femoral-acetabular displacement as an objective indicator of instability. To evaluate this potential, 10 patients indicated for periacetabular osteotomy to treat hip dysplasia and 10 healthy controls underwent two WBCT protocols. Participants were scanned in a neutral stance [weight-bearing (WB)] and again with the hip stressed in maximal external rotation (WB-stress), a position hypothesized to reproduce anterior instability. Clinical, nonweight-bearing computed tomography (CT) scans were available for patients with hip dysplasia. Congruency of the femoroacetabular joint space and position of the femoral head in the acetabulum were quantified via multiple 2D manual measurements and automated 3D measurements. There were no 2D measurements found to differ between the WB and WB-stress scans in either dysplastic (P = .742-1.000) or control (P = .203-1.000) hips. 3D translation of the femoral head center from WB to WB-stress averaged 1.3 ± 0.6 mm in the control hips, compared to 0.9 ± 0.4 mm in the dysplastic hips (P = .096). 3D joint space width (JSW) was determined for both the control and dysplastic hips, with greater JSW found in control hips for both the WB (P = .049) and WB-stress (P = .003) scans. WBCT has the potential to better capture subtle femoral-acetabular displacement derived from both automated 3D and manual 2D measurements in static instability-prone joint orientations.
© The Author(s) 2025. Published by Oxford University Press.
Conflict of interest statement
No author has any relevant conflict of interests with this work to declare.
Figures
References
-
- Willey MC, Westermann RW Glass N et al. Risk factors for composite failure of hip dysplasia treated with periacetabular osteotomy: a minimum 10-year follow-up. J Am Acad Orthop Surg 2022;30:e690–e702. - PubMed
LinkOut - more resources
Full Text Sources
