

Case Report: Extracorporeal photopheresis for BK virus nephropathy as a novel treatment for high-risk rejection kidney transplant recipient
- PMID: 40761768
- PMCID: PMC12318737
- DOI: 10.3389/fneph.2025.1625060
Case Report: Extracorporeal photopheresis for BK virus nephropathy as a novel treatment for high-risk rejection kidney transplant recipient
Abstract
Background: BK virus-associated nephropathy (BKVAN) is a major complication in kidney transplantation caused by the reactivation of latent BK virus (BKV) under immunosuppression. BKVAN has been strongly associated with increased graft loss. Currently, there is no effective antiviral treatment for BKVAN. Additionally, the development of donor-specific antibodies (DSAs) and the risk of acute and chronic rejection complicate the reduction of immunosuppressive therapy (IS). This case report illustrates the management of BKVAN in a highly sensitized transplant recipient and explores the potential use of extracorporeal photopheresis (ECP) as an immunomodulatory tool.
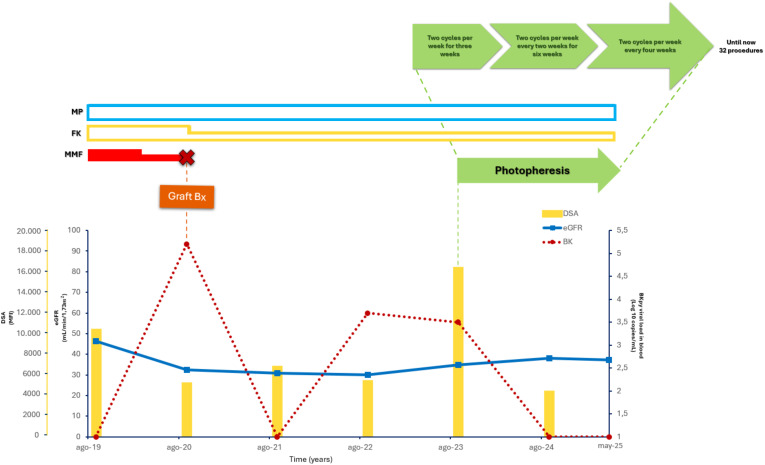
Case: 44-year-old Caucasian woman with a history of failed prior transplant and multiple transfusions underwent a second kidney transplant. Due to a high panel-reactive antibody level, she received induction therapy with plasma exchange, thymoglobulin and steroids, followed by maintenance with tacrolimus, mycophenolate mofetil (MMF), and steroids. Initial graft function was good, and protocol biopsies showed no rejection. In year four, the patient developed an increasing BKV viremia (peak of 40,050 copies/mL) and MMF was reduced, which cleared BKV in six months. Two years later, DSAs reappeared, which led to an increase in MMF. In August 2020 the patient showed a decline of GFR, elevated BKV viremia (peak 162,000 copies/mL), and a graft biopsy was performed revealing BKVAN. IS was reduced (MMF was discontinued, and tacrolimus was tapered). After eight months, the viremia cleared up, but anti-DR53 DSAs (MFI 16000) levels increased significantly. As the patient was highly sensitized and had a thrombosis of arteriovenous fistula, mTOR inhibitors were not recommended. In order to modulate alloimmunity without further suppressing antiviral immunity, ECP was introduced. Over the next two years, the patient showed stable renal function (eGFR 30-40 mL/min), no recurrence of BKV viremia, and a gradual reduction in DSAs titers. No acute rejection episodes occurred.
Conclusions: In a highly sensitized patient with BKVAN and contraindications to standard therapies, ECP combined with a tailored immunosuppressive regimen proved effective in controlling viral replication, preserving graft function, and mitigating alloimmune risks. Considering the potential of ECP as an adjunctive therapy in complex BKVAN scenarios, further investigation is warranted.
Keywords: BK virus; BKVAN; ECP; antibody mediated rejection; high sensitized; kidney transplantation.
Copyright © 2025 Gregorini, Del Fante, Islami, Grignano, Serpieri, Perotti, Viarengo, Locurcio, Lanotte, Tragni, Stea, Martinelli, Marchi, Portalupi, De Mauri, Margiotta, Pattonieri, Soccio and Rampino.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Interventions for BK virus infection in kidney transplant recipients.Cochrane Database Syst Rev. 2024 Oct 9;10(10):CD013344. doi: 10.1002/14651858.CD013344.pub2. Cochrane Database Syst Rev. 2024. PMID: 39382091
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.Health Technol Assess. 2006 Dec;10(49):iii-iv, ix-xi, 1-157. doi: 10.3310/hta10490. Health Technol Assess. 2006. PMID: 17134597
-
Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation: a systematic review and modelling study.Health Technol Assess. 2005 May;9(21):1-179, iii-iv. doi: 10.3310/hta9210. Health Technol Assess. 2005. PMID: 15899149
-
Polyclonal and monoclonal antibodies for treating acute rejection episodes in kidney transplant recipients.Cochrane Database Syst Rev. 2017 Jul 20;7(7):CD004756. doi: 10.1002/14651858.CD004756.pub4. Cochrane Database Syst Rev. 2017. PMID: 28731207 Free PMC article.
-
Polyclonal and monoclonal antibodies for induction therapy in kidney transplant recipients.Cochrane Database Syst Rev. 2017 Jan 11;1(1):CD004759. doi: 10.1002/14651858.CD004759.pub2. Cochrane Database Syst Rev. 2017. PMID: 28073178 Free PMC article.
References
-
- Wong ASY, Cheng VCC, Yuen KY, Kwong YL, Leung AYH. High frequency of polyoma BK virus shedding in the gastrointestinal tract after hematopoietic stem cell transplantation: a prospective and quantitative analysis. Bone Marrow Transplant. (2009) 43:43–7. doi: 10.1038/bmt.2008.266, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous