

A Rare Case of Intracranial Hemorrhage Mimicking a Neoplasm in a Child With Hereditary Hemorrhagic Telangiectasia
- PMID: 40761947
- PMCID: PMC12321042
- DOI: 10.7759/cureus.87340
A Rare Case of Intracranial Hemorrhage Mimicking a Neoplasm in a Child With Hereditary Hemorrhagic Telangiectasia
Abstract
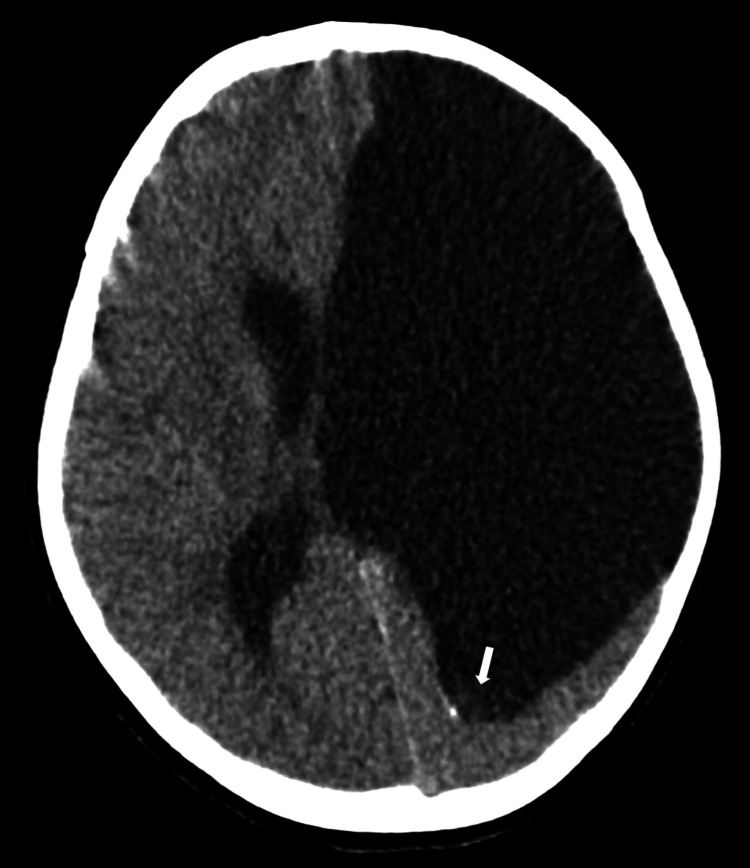
Hereditary hemorrhagic telangiectasia (HHT) is an autosomal dominant disorder characterized by abnormal blood vessel formation, resulting in the development of arteriovenous malformations and telangiectasias throughout the body. We present a rare case of an intracranial hemorrhage mimicking a neoplasm in a medically complex pediatric patient with HHT, a diagnosis that was unbeknownst to both the clinical team and the interpreting radiologist early in the patient's clinical course. This case not only demonstrates the importance of obtaining a thorough medical history but having a clear understanding of the numerous manifestations of HHT, especially as it pertains to the pediatric population. We implore strictly adhere to the guidelines of brain imaging at the time of diagnosis, as well as a multidisciplinary approach to the surveillance and management of these patients in hopes of preventing serious and potentially fatal complications.
Keywords: arteriovenous malformation; hereditary hemorrhagic telangiectasia (hht); neuroradiology; osler-weber-rendu syndrome; pediatric radiology; vascular malformations.
Copyright © 2025, Solano et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures




References
-
- Epidemiology and trends of hereditary hemorrhagic telangiectasia in the United States. Ferry AM, Wright AE, Baillargeon G, Kuo YF, Chaaban MR. Am J Rhinol Allergy. 2020;34:230–237. - PubMed
-
- Diagnostic criteria for hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome) Shovlin CL, Guttmacher AE, Buscarini E, et al. Am J Med Genet. 2000;91:66–67. - PubMed
-
- International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. Faughnan ME, Palda VA, Garcia-Tsao G, et al. J Med Genet. 2011;48:73–87. - PubMed
-
- Second international guidelines for the diagnosis and management of hereditary hemorrhagic telangiectasia. Faughnan ME, Mager JJ, Hetts SW, et al. Ann Intern Med. 2020;173:989–1001. - PubMed
Publication types
LinkOut - more resources
Full Text Sources