

doi: 10.1177/19714009251362825.
Online ahead of print.
High grade torcular DAVF: Technical aspects to safely sacrifice the straight sinus
Affiliations
- PMID: 40762170
- PMCID: PMC12325241
- DOI: 10.1177/19714009251362825
Item in Clipboard
High grade torcular DAVF: Technical aspects to safely sacrifice the straight sinus
Neuroradiol J.
.
Abstract
High grade torcular DAVFs can be challenging to treat, particularly when there is retrograde flow in the straight sinus and deep venous system. We describe the technical steps to safely sacrifice the straight sinus, including preoperative MRI findings, arterial and venous cerebral flow assessment and key points for endovascular treatment.
Keywords: DAVF; Dural arteriovenous fistula; embolization; isolated DAVF; isolated dural arteriovenous fistula; isolated sinus; surgery.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
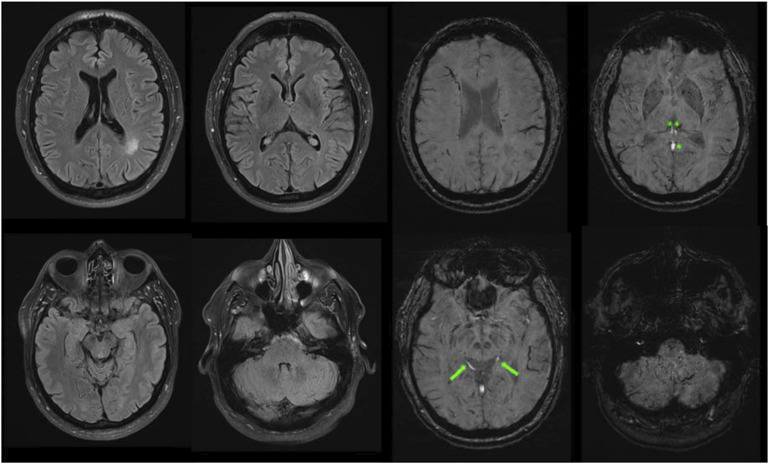
3.0 T axial T2 FLAIR images (left) demonstrate absence of vasogenic edema in the thalami, basal ganglia and periventricular white matter, as well as a small area with vasculo-ischemic white matter changes in the left parietal deep white matter. Axial SWI images (right) show arterialized (hyperintense) signal in the deep venous system, including the internal cerebral veins (double asterisks), vein of Galen (asterisk) and basal veins of Rosenthal (arrows).
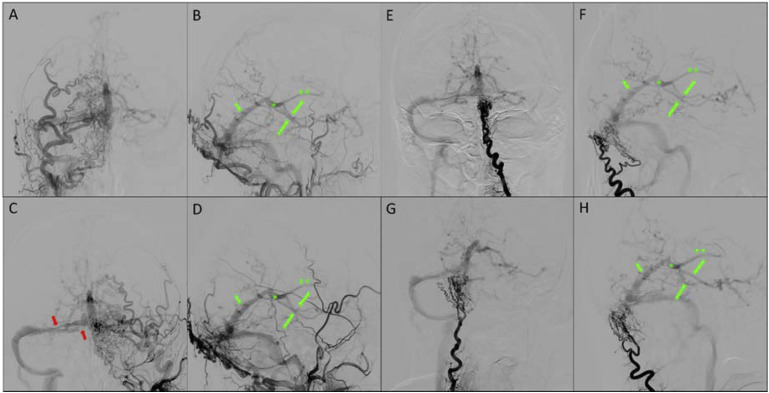
Preoperative cerebral angiogram demonstrates a multihole high grade DAVF at the torcular. AP (A, C) and lateral injections (B, D) of the external carotid arteries demonstrate innumerable hypertrophic arterial feeders from the occipital arteries (transosseous branches), and minor supply from the middle meningeal arteries, posterior auricular and posterior meningeal arteries. AP (E, G) and lateral (F, H) injection of the deep cervical arteries show additional transosseous feeders. There is reflux into the straight sinus (small arrow), vein of Galen (asterisk), internal cerebral veins (asterisks), basal veins of Rosenthal (arrows) as cerebral and cerebellar cortical veins. The torcular is disconnected from the superior sagittal sinus and left transverse sinus and demonstrates high grade stenotic channels (red arrows) with the right transverse sinus.
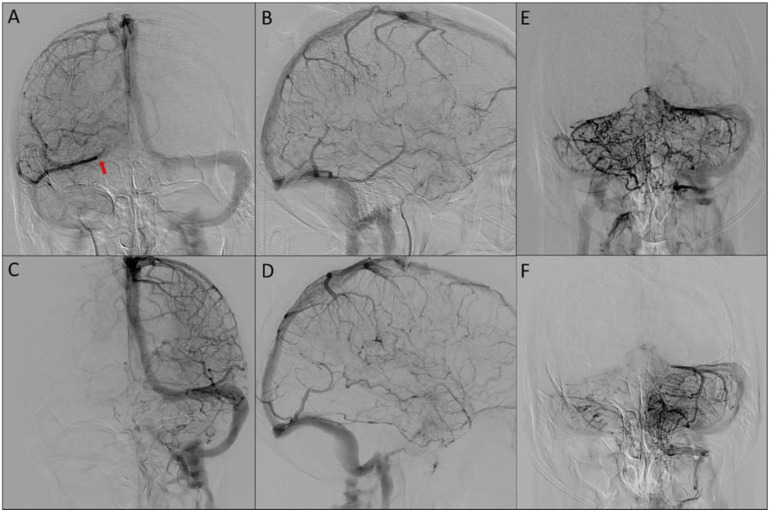
AP (A,C) and lateral (B,D) venograms of the right and left hemisphere, respectively and AP venograms of the right (E) and left (F) vertebral artery injections demonstrate normal patency of the left-sided dural venous system. The straight sinus is not used for normal venous drainage of the cerebral and cerebellar hemispheres. The cerebral hemispheres primarily demonstrate centrifugal venous drainage of the deep white matter towards the cortex. The right vein of Labbe demonstrates persistent drainage into the right proximal transverse sinus (arrow) close to the DAVF and deserves balloon protection during embolization.
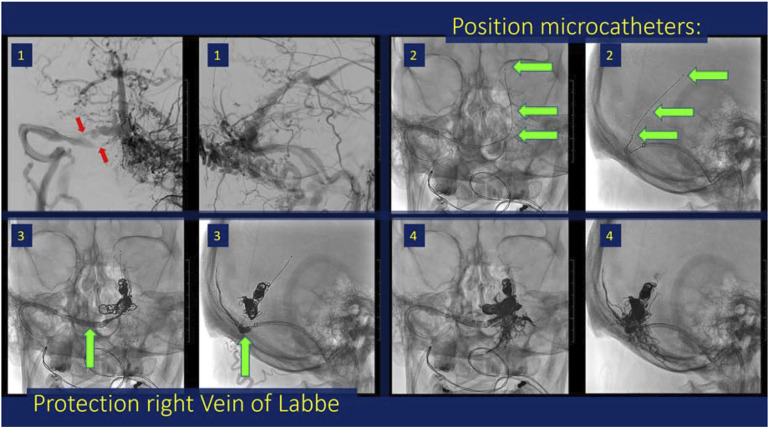
Technical steps of endovascular treatment. Working projections (1) demonstrate the 8 Fr guide catheter in the right distal transverse sinus via right internal jugular access for optimal support. Three Echelon 10 microcatheter were navigated via the inferior high grade stenotic lumen into the affected sinus segment (inferior red arrow). The microcatheters were positioned in staggered fashion (2) in the proximal straight sinus close to the vein of Galen, at the mid portion of the straight sinus and in the torcular (green arrows). A 6 × 20 mm Eclipse balloon was inflated protecting the outflow trajectory of the right vein of Labbe during Onyx embolization (3) resulting in closure of the interstices in between the coil mesh (4).
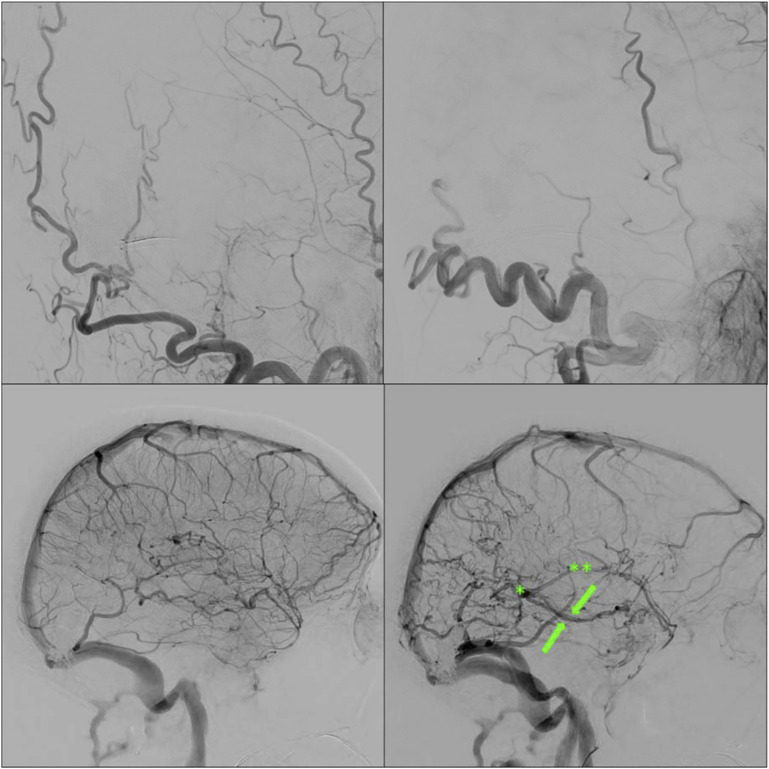
Direct postoperative angiogram demonstrated complete closure of the DAVF on right ECA (left upper) and left ECA (right upper) injections. Venograms of the left ICA (left lower) and right ICA (right lower) demonstrate persistent non-opacification of the straight sinus. There is immediate normalization of venous drainage of the deep venous system, including the internal cerebral veins (asterisks), vein of Galen (asterisk) and basal veins of Rosenthal (arrows).
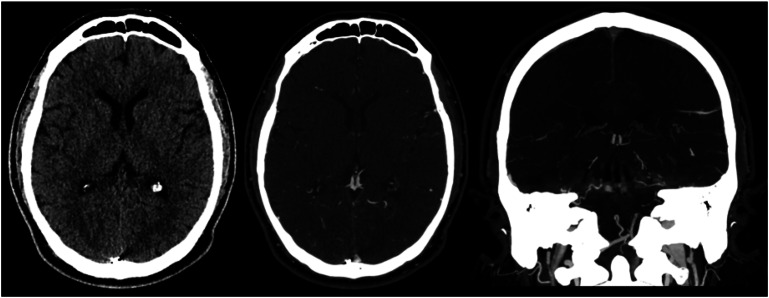
Delayed CT venogram after 6 weeks demonstrates unremarkable aspect of the brain parenchyma and patency of the deep venous system.
Similar articles
-
Bilateral Thalamic Edema Caused by Tentorial Galenic Dural Arteriovenous Fistula and Sinus Thrombosis: Successful Endovascular Therapy.Turk Neurosurg. 2025;35(4):667-671. doi: 10.5137/1019-5149.JTN.47423-24.1. Turk Neurosurg. 2025. PMID: 40577497
-
Parasagittal and Superior Sagittal Sinus Dural Arteriovenous Fistulas: Clinical Presentations, Imaging Characteristics, and Treatment Strategies.AJNR Am J Neuroradiol. 2024 Aug 9;45(8):1025-1030. doi: 10.3174/ajnr.A8246. AJNR Am J Neuroradiol. 2024. PMID: 38479780 Free PMC article.
-
Dural arteriovenous fistulas of the hypoglossal canal: systematic review on imaging anatomy, clinical findings, and endovascular management.J Neurosurg. 2015 Apr;122(4):883-903. doi: 10.3171/2014.10.JNS14377. Epub 2014 Nov 21. J Neurosurg. 2015. PMID: 25415064
-
Superior sagittal sinus dural arteriovenous fistulas: navigating the complexity of treatment strategies and outcomes.J Clin Neurosci. 2025 Aug 6;140:111544. doi: 10.1016/j.jocn.2025.111544. Online ahead of print. J Clin Neurosci. 2025. PMID: 40773855
-
De Novo dural arteriovenous fistulas after endovascular treatment: Case illustration and literature review.Interv Neuroradiol. 2024 Aug;30(4):597-603. doi: 10.1177/15910199221118517. Epub 2022 Aug 4. Interv Neuroradiol. 2024. PMID: 35924383 Free PMC article. Review.
References
-
- van Dijk JM, terBrugge KG, Willinsky RA, et al. Clinical course of cranial dural arteriovenous fistulas with long-term persistent cortical venous reflux. Stroke 2002; 33: 1233–1236. - PubMed
-
- Osada T, Krings T. Intracranial dural arteriovenous fistulas with pial arterial supply. Neurosurgery 2019; 84: 104–115. - PubMed
LinkOut - more resources
Full Text Sources
