

Eradicating Drug-tolerant Persister Cells in EGFR-Mutated Non-Small Cell Lung Cancer by Targeting TROP2 with CAR-T Cellular Therapy
- PMID: 40762432
- PMCID: PMC12374242
- DOI: 10.1158/2159-8290.CD-24-1515
Eradicating Drug-tolerant Persister Cells in EGFR-Mutated Non-Small Cell Lung Cancer by Targeting TROP2 with CAR-T Cellular Therapy
Abstract
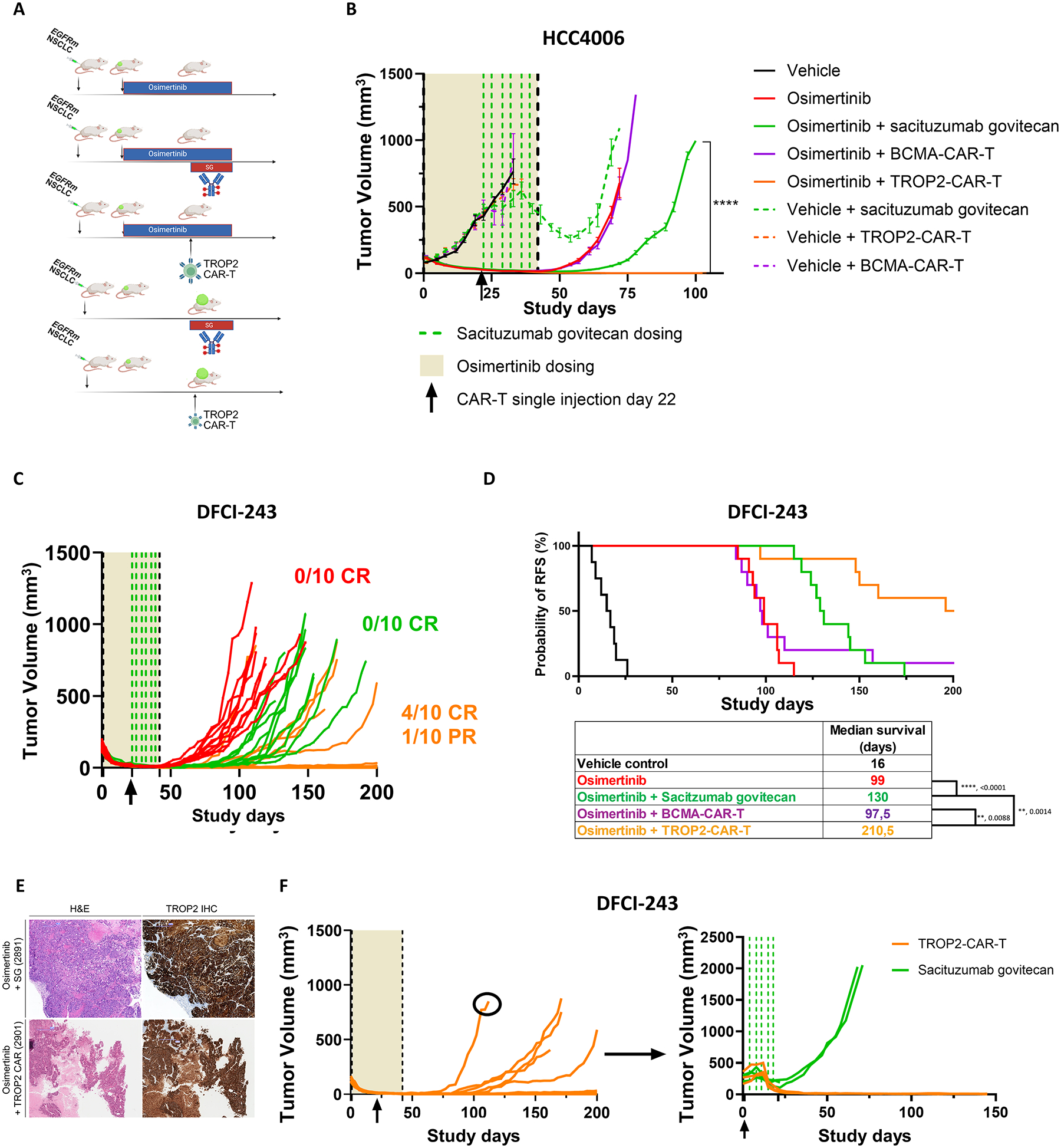
EGFR tyrosine kinase inhibitors have dramatically improved outcomes for patients with EGFR-mutated non-small cell lung cancer (NSCLC), but relapse frequently occurs because of drug-tolerant persister (DTP) cells that can evolve and develop diverse mechanisms of drug resistance. In samples from patients with EGFR-mutated NSCLC treated with EGFR tyrosine kinase inhibitors in the neoadjuvant setting, we observed enriched expression of the cell surface protein TROP2, a target of clinically active antibody-drug conjugates (ADC). We confirmed these findings across multiple EGFR-mutated NSCLC cell line and patient-derived xenograft models treated with osimertinib in vivo. Treatment with the TROP2 ADC sacituzumab govitecan at the time of osimertinib-induced minimal residual disease only modestly delayed tumor recurrence in vivo, whereas a single infusion of sacituzumab-based TROP2-directed chimeric antigen receptor (CAR) T cells significantly prolonged relapse-free survival, with evidence of cure. These data highlight the potential of engineering TROP2 CAR T-cell therapy to eliminate EGFR DTPs in patients.
Significance: We provide a rationale for targeting TROP2 in EGFR-mutated NSCLC DTPs. In contrast to TROP2 ADC therapy, targeting of TROP2 with CAR-T cells can eliminate osimertinib-induced DTPs in vivo, revealing the promise of developing novel TROP2-based CAR-T cells to promote durable response and prevent disease relapse in patients.
©2025 American Association for Cancer Research.
Conflict of interest statement
D.A.B. is a consultant for N of One/Qiagen and Nerviano Medical Sciences, is a founder and shareholder in Xsphera Biosciences, has received honoraria from Merck, H3 Biomedicine/Esai, EMD Serono, Gilead Sciences, Abbvie, and Madalon Consulting, and research grants from BMS, Takeda, Novartis, Gilead, and Lilly.
E.L.S. is a consultant for Bristol-Myers Squibb, Chimeric Therapeutics, Chroma Medicine, Eureka Therapeutics, Sana Biotech, and Secura Bio, Inc. He has received research grants from Sanofi Pasteur Biologics LLC, holds patents for antibodies targeting GPRC5D, and CAR-T cells targeting BCMA and GPRC5D. E.L.S and E.J.B are inventors on a pending patent for CARs targeting TROP2.
P.A.J. has stock and other ownership interests in Gatekeeper Pharmaceuticals. He serves as a consultant or advisor for Pfizer, Boehringer Ingelheim, AstraZeneca, Merrimack, Chugai Pharma, Roche/Genentech, LOXO, Mirati Therapeutics, Araxes Pharma, Ignyta, Lilly, Takeda, Novartis, Biocartis, Voronoi Health Analytics, SFJ Pharmaceuticals Group, Sanofi, Daiichi Sankyo, Silicon Therapeutics, Nuvalent, Inc, Eisai, Bayer, Syndax, AbbVie, Allorion Therapeutics, Accutar Biotech, Transcenta, Monte Rosa Therapeutics, Scorpion Therapeutics, Merus, Frontier Medicines, Hongyun Biotech, Duality Biologics, Dizal Pharmaceuticals, GlaxoSmithKline, Tolremo and Myris Therapeutics.Blueprint. He has received research funding from AstraZeneca, Astellas Pharma, Daiichi Sankyo, Lilly, Boehringer Ingelheim, Puma Biotechnology, Takeda, and Revolution Medicines (all institutionally). He is a co-inventor on a DFCI-owned patent on EGFR mutations licensed to LabCorp and receives post-marketing royalties from this invention.
S.B. has received funding for participation in training courses, congresses and expert group meetings from Pfizer, Roche, GSK, Lilly, MSD, Boehringer Ingelheim, Amgen, Janssen, and AstraZeneca.
F.F. has received personal fees from Roche for speaker activity.
Figures



References
-
- Soria J-C, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in Untreated EGFR -Mutated Advanced Non–Small-Cell Lung Cancer. New England Journal of Medicine. 2018;378:113–25. - PubMed
-
- Planchard D, Jänne PA, Cheng Y, Yang JC-H, Yanagitani N, Kim S-W, et al. Osimertinib with or without Chemotherapy in EGFR-Mutated Advanced NSCLC. New England Journal of Medicine. Massachusetts Medical Society; 2023;389:1935–48. - PubMed
-
- Cho BC, Lu S, Felip E, Spira AI, Girard N, Lee J-S, et al. Amivantamab plus Lazertinib in Previously Untreated EGFR-Mutated Advanced NSCLC. N Engl J Med. 2024;391:1486–98. - PubMed
MeSH terms
Substances
Grants and funding
- LUNGSTRONG
- CRP-17-111-01-CDD/American Cancer Society (ACS)
- NIH R01CA190294/National Cancer Institute (NCI)
- N°AAPMRC2.2020.LCC/SB/La Ligue contre le cancer
- Polly and Ming Tsai Lung Cancer Research Fund
- Angela Marotta Inho Foundation
- Ludwig Center at Harvard Medical School
- Kaifer Family Fund
- P50 CA265826/CA/NCI NIH HHS/United States
- Heerwagen Family Fund for Lung Cancer Research
- K08 CA270077/CA/NCI NIH HHS/United States
- NIH R01CA293092/National Cancer Institute (NCI)
- Chen-Huang Center for EGFR Mutant Lung Cancers
- R01 CA190394/CA/NCI NIH HHS/United States
- Candice Bagby Fund
- Team 3G
- LUNGevity Foundation (LUNGevity)
- R01 CA293092/CA/NCI NIH HHS/United States
- NIH K08CA270077/National Cancer Institute (NCI)
- Lubin Family Foundation Scholar Award
- Lung SPORE P50CA265826/National Cancer Institute (NCI)
- R35 CA220497/CA/NCI NIH HHS/United States
- IASLC -LCRF Team Science Research Grant/International Association for the Study of Lung Cancer (IASLC)
- Philippe Foundation Inc
- The Jaksaa Fund
- Robert Weyland Henkel Fund for Lung Cancer Research
- Parker Institute for Cancer Immunotherapy (PICI)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
