

HEV seroprevalence and associated risk factors among HIV-positive individuals in post-earthquake Kathmandu: a 2016 cross-sectional study
- PMID: 40764531
- PMCID: PMC12326692
- DOI: 10.1186/s12879-025-11382-8
HEV seroprevalence and associated risk factors among HIV-positive individuals in post-earthquake Kathmandu: a 2016 cross-sectional study
Abstract
Introduction: Hepatitis E virus (HEV) infection poses a significant public health challenge, particularly in immunocompromised populations such as those living with HIV. Limited data exist on HEV seroprevalence and its correlates among HIV-positive individuals in urban low-resource settings, especially in the aftermath of disasters. This study investigates HEV seroprevalence and risk factors among HIV positive individuals in 2016, a post-earthquake period in Kathmandu, Nepal, with relevance to ongoing challenges in 2025.
Methods: We conducted a cross-sectional serological study among 200 HIV-positive individuals from Sukraraj Tropical and Infectious Disease Hospital's (STIDH) Antiretroviral Therapy (ART) center in Kathmandu. Serological testing determined anti-HEV IgG and IgM status using Wantai Hepatitis E (HEV-IgG/M) ELISA kits. Sociodemographic, behavioral, and clinical data were collected via structured interviews and medical records. Multivariable logistic regression identified independent predictors of anti-HEV IgG seropositivity. Statistical analyses used Chi-square, Mann-Whitney U, and Cochran's Q tests, with p < 0.05 considered significant. A comparative general population sample (n = 100) from earthquake-affected districts was also analyzed.
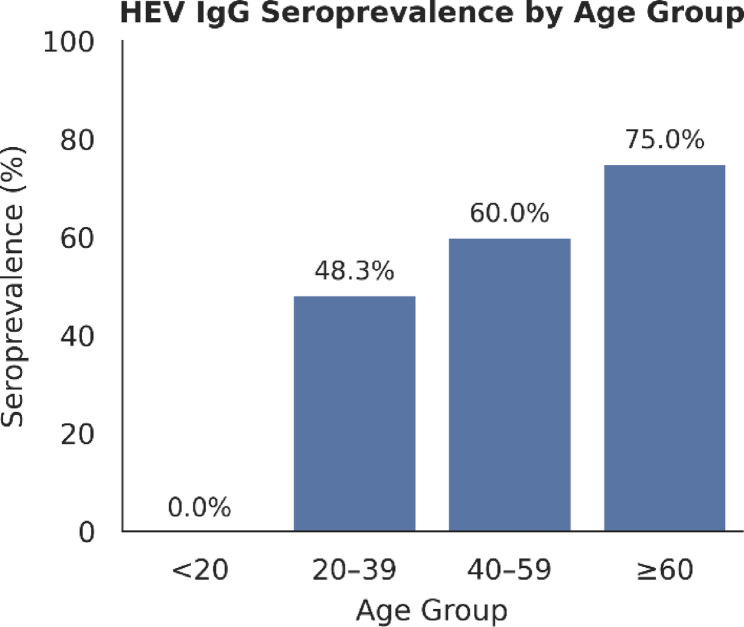
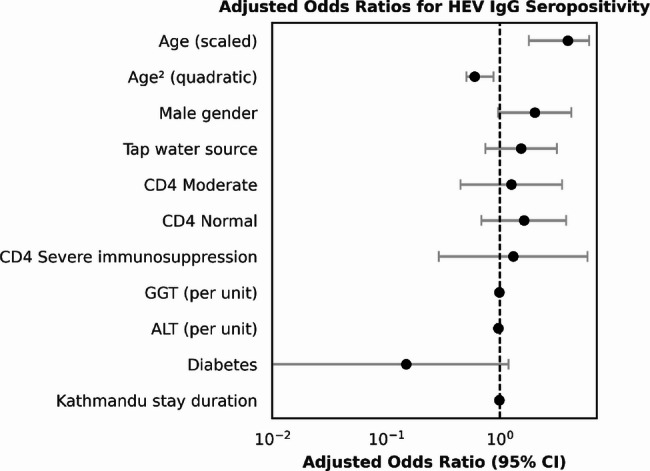
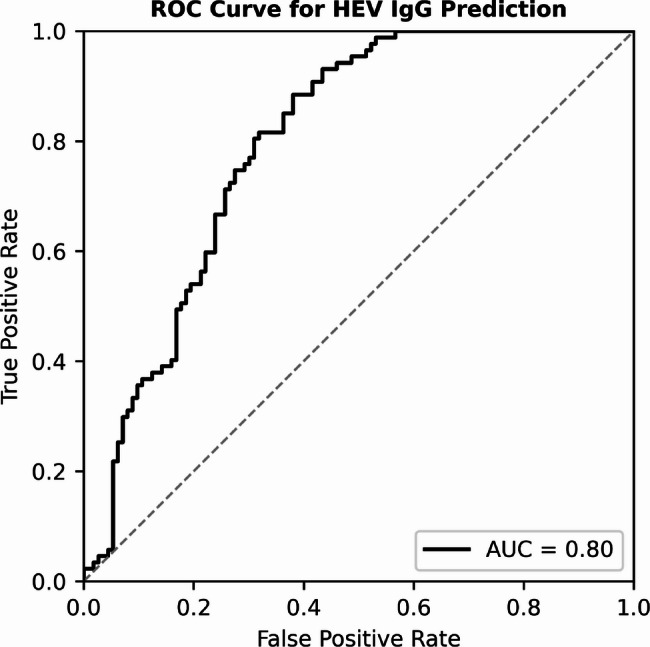
Results: Overall, 43.5% (87/200) of HIV-positive participants tested positive for anti-HEV IgG. Key demographic predictors included increasing age, which showed a significant non-linear association (adjusted OR = 3.95 for age, 0.60 for age²; p < 0.001), and a marginal association with male gender (aOR = 2.03; p = 0.059). In contrast, no significant associations were observed between HEV seropositivity and specific drinking water sources, water processing methods, eating habits, smoking status, CD4 count, HIV viral load suppression, common comorbidities, or routine liver and hematological markers. anti-HEV IgG seroprevalence was considerably higher than that of Hepatitis B virus (4.5%) and Hepatitis C virus (5.0%) in the cohort and notably absent in a comparative general population sample. The predictive model showed good performance (AUC = 0.80), supporting its exploratory utility.
Conclusion: Our findings reveal a high burden of past HEV exposure among HIV-positive individuals in post-earthquake Kathmandu, with age being a key correlate. The absence of HEV IgG positivity in the general population sample suggests that HEV exposure during this period may have been localized to vulnerable clinical groups. The lack of association with traditional behavioral or clinical markers highlights the complexity of transmission in this setting. These results underscore the need to integrate HEV awareness and targeted screening into HIV care in endemic regions. Future studies should prioritize longitudinal follow-up, genotype surveillance, and environmental sampling to inform public health preparedness and response.
Keywords: HIV-positive; Hepatitis E virus (HEV); Kathmandu; Post-earthquake; Seroprevalence.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Ethics committee of Nepal Health Research Council, Kathmandu, Nepal (Approval No. 172). Informed consent was obtained from all participants or their guardians, and participants confidentiality was maintained through data anonymization. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Clinical trial number: Not applicable.
Figures
Similar articles
-
The Epidemiology of Hepatitis E in Israel and Potential Risk Factors: A Cross-Sectional Population-Based Serological Survey of Hepatitis E Virus in Northern Israel.Viruses. 2025 Apr 7;17(4):536. doi: 10.3390/v17040536. Viruses. 2025. PMID: 40284979 Free PMC article.
-
Higher Hepatitis E Seroprevalence in Workers in the Pig Sector in Flanders, Belgium: Results From a Seroprevalence Case-Control Study.Zoonoses Public Health. 2025 Aug;72(5):442-452. doi: 10.1111/zph.13223. Epub 2025 May 2. Zoonoses Public Health. 2025. PMID: 40317906
-
Heterogeneity in the seroprevalence of hepatitis E virus among hospital attendees: a retrospective study in Shanghai, China.Infect Dis (Lond). 2025 Jul;57(7):647-657. doi: 10.1080/23744235.2025.2471819. Epub 2025 Feb 27. Infect Dis (Lond). 2025. PMID: 40017260
-
Antibody tests for identification of current and past infection with SARS-CoV-2.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD013652. doi: 10.1002/14651858.CD013652.pub2. Cochrane Database Syst Rev. 2022. PMID: 36394900 Free PMC article.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
References
-
- World Health Organization, Hepatitis E. 2025. https://www.who.int/news-room/fact-sheets/detail/hepatitis-e. Accessed 30 May 2025.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
