

Enhancing pediatric distal radius fracture detection: optimizing YOLOv8 with advanced AI and machine learning techniques
- PMID: 40764539
- PMCID: PMC12326825
- DOI: 10.1186/s12880-025-01669-2
Enhancing pediatric distal radius fracture detection: optimizing YOLOv8 with advanced AI and machine learning techniques
Abstract
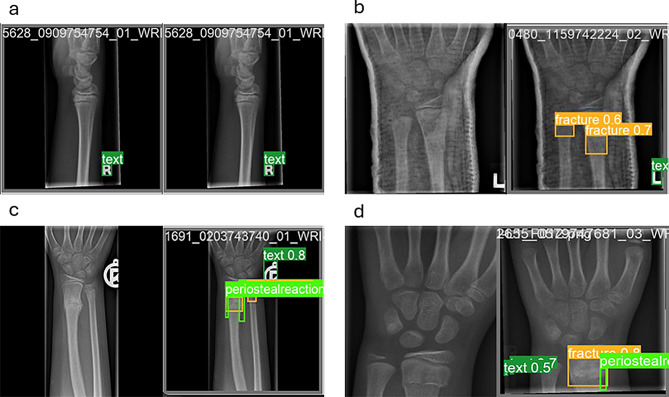
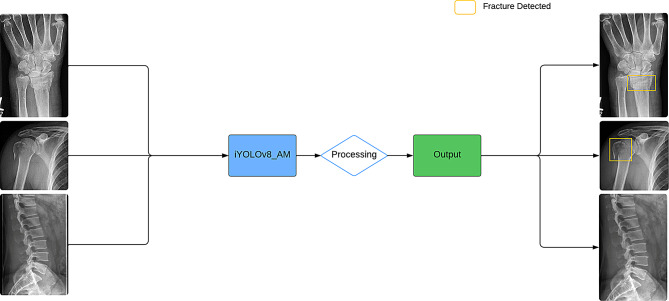
Background: In emergency departments, residents and physicians interpret X-rays to identify fractures, with distal radius fractures being the most common in children. Skilled radiologists typically ensure accurate readings in well-resourced hospitals, but rural areas often lack this expertise, leading to lower diagnostic accuracy and potential delays in treatment. Machine learning systems offer promising solutions by detecting subtle features that non-experts might miss. Recent advancements, including YOLOv8 and its attention-mechanism models, YOLOv8-AM, have shown potential in automated fracture detection. This study aims to refine the YOLOv8-AM model to improve the detection of distal radius fractures in pediatric patients by integrating targeted improvements and new attention mechanisms.
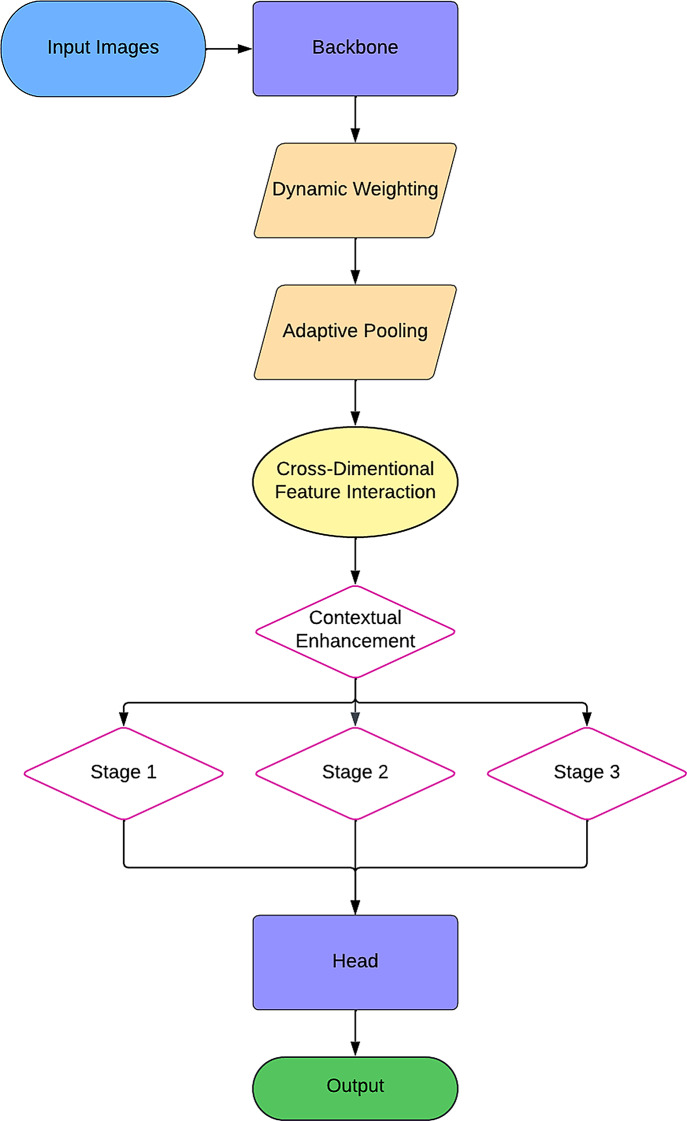
Methods: We enhanced the YOLOv8-AM model to improve pediatric wrist fracture detection, maintaining the YOLOv8 backbone while integrating attention mechanisms such as the Convolutional Block Attention Module (CBAM) and the Global Context (GC) block. We optimized the model through hyperparameter tuning, implementing data cleaning, augmentation, and normalization techniques using the GRAZPEDWRI-DX dataset. This process addressed class imbalances and significantly improved model performance, with mean Average Precision (mAP) increasing from 63.6 to 66.32%.
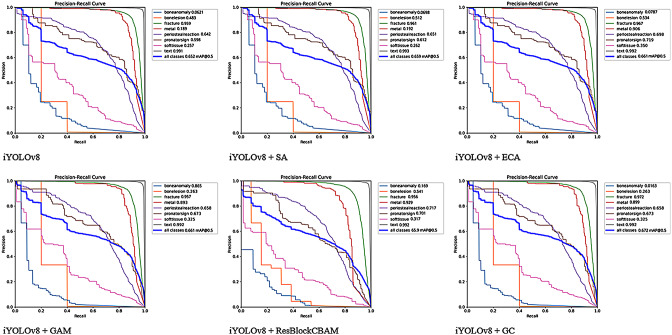
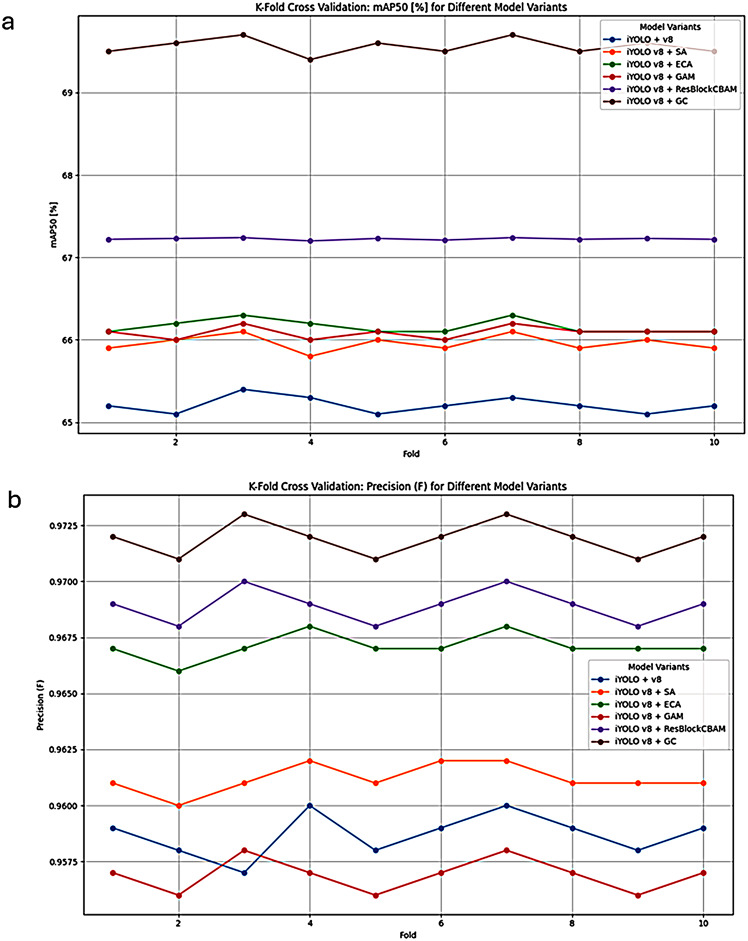
Results and discussion: The iYOLOv8 models demonstrated substantial improvements in performance metrics. The iYOLOv8 + GC model achieved the highest precision at 97.2%, with an F1-score of 67% and an mAP50 of 69.5%, requiring only 3.62 h of training time. In comparison, the iYOLOv8 + ECA model reached 96.7% precision, significantly reducing training time from 8.54 to 2.16 h. The various iYOLOv8-AM models achieved an average accuracy of 96.42% in fracture detection, although performance for detecting bone anomalies and soft tissues was lower due to dataset constraints. The improvements highlight the model's effectiveness in pathological detection of the pediatric distal radius, suggesting that integrating these AI models into clinical practice could significantly enhance diagnostic efficiency.
Conclusion: Our improved YOLOv8-AM model, incorporating the GC attention mechanism, demonstrated superior speed and accuracy in pediatric distal radius fracture detection while reducing training time. Future research should explore additional features to further enhance detection capabilities in other musculoskeletal areas, as this model has the potential to adapt to various fracture types with appropriate training.
Clinical trial number: Not applicable.
Keywords: AI and wrist fracture; Automated detection; Convolution block attention module (CBAM); Distal and radius fracture; Global context block; Pediatric fracture; YOLOv8-AM.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable, since the study includes de-identified data available online. Consent for publication: Not applicable, since the study includes de-identified data available online. Competing interests: The authors declare no competing interests.
Figures

References
-
- Miele V, Galluzzo M, Trinci M. Missed fractures in the emergency department. In: Romano L, Pinto A, editors. Errors in radiology. Milano: Springer Milan; 2012. pp. 39–50.
-
- Rimmer A. Radiologist shortage leaves patient care at risk, warns Royal college. BMJ. 2017;359:j4683. - PubMed
-
- Berlin L. Defending the missed radiographic diagnosis. AJR Am J Roentgenol. 2001;176:317–22. - PubMed
-
- Mounts J, Clingenpeel J, McGuire E, Byers E, Kireeva Y. Most frequently missed fractures in the emergency department. Clin Pediatr (Phila). 2011;50:183–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
