

Core competency model self-directed violence prevention training program for corrections: a hybrid feasibility-effectiveness trial
- PMID: 40764547
- PMCID: PMC12326600
- DOI: 10.1186/s12889-025-23853-3
Core competency model self-directed violence prevention training program for corrections: a hybrid feasibility-effectiveness trial
Abstract
Background: Self-directed violence encompasses both suicide and self-injury. United States correctional settings face high self-directed violence rates. Training correctional behavioral health clinicians (BHCs) in evidence-based self-directed violence prevention practices represents one solution. The Core Competency Model for Corrections (CCM-C) is a self-directed violence prevention training program addressing clinician self-management (e.g., managing personal reactions to self-directed violence) and clinical care (e.g., eliciting evidence-based risk and protective factors) skills. The present study held aims to: (1) assess CCM-C feasibility, appropriateness, acceptability, and usability; (2) evaluate short-term impacts on BHC self-directed violence knowledge, attitudes, and skill usage; and (3) explore short-term impacts on BHC compassion fatigue.
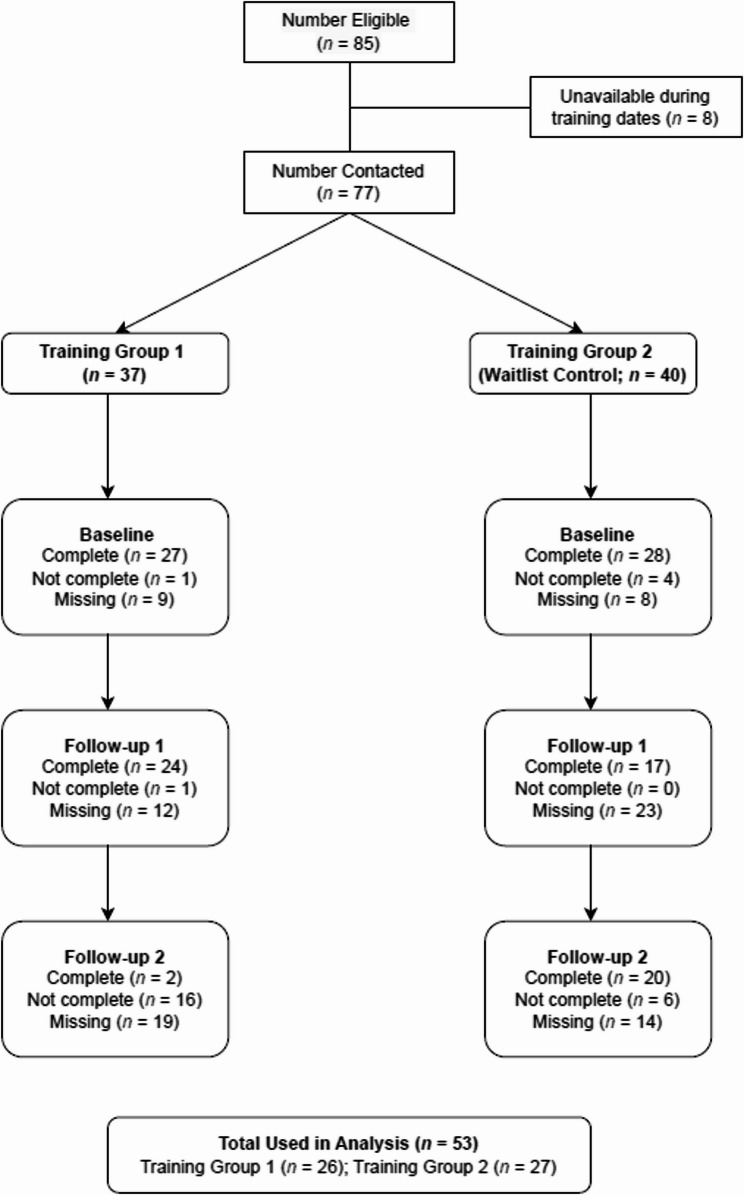
Methods: The present study was a statewide hybrid feasibility-effectiveness trial evaluating the CCM-C taking place between January and December 2024. Pre-training feedback was gathered from a corrections advisory panel (N = 7). For the trial implementation, we conducted a waitlist control sequential cross-over design. BHCs (N = 60) were randomly assigned to two training groups: Baseline training versus waitlist control. BHCs provided quantitative and qualitative survey input on CCM-C feasibility outcomes (aim 1), and completed self-report inventories of self-directed violence-related outcomes (aims 2 and 3). Descriptive statistics and thematic analysis assessed feasibility outcomes. Repeated-measures analysis of variance (ANOVA) tests examined CCM-C outcomes.
Results: CCM-C was highly acceptable, appropriate, feasible, and usable. Recommended improvements included removing non-corrections content, enhancing opportunities for BHC participation and interaction, and creating participant handout packages. CCM-C increased BHC self-directed violence prevention knowledge, perceived skill mastery, intent/actual use of training content, and lowered compassion fatigue levels. Attitudes toward intervening with a suicidal person only improved for the waitlist control group. Attitudes towards incarcerated individuals who self-harm remained unchanged.
Discussion: Early results show CCM-C to be a feasible, effective self-directed violence prevention training program for correctional BHCs. Results support broader CCM training literature and a social-cognitive training model. Statewide partners will generate the CCM-C Toolkit, a package comprising training materials, implementation guidance, and train-the-trainer materials. The Toolkit will provide accessible resources for further CCM-C implementation, adaptation, and evaluation.
Trial registration: This study was registered at clinicaltrials.gov (NCT06359574).
Keywords: Clinician; Corrections; Self-directed violence; Self-injury; Suicide; Training.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the UNC Charlotte Institutional Review Board (IRB) in compliance with the Declaration of Helsinki and with all applicable Federal regulations governing the protection of human subjects. All participants affirmed consent via the IRB-approved e-informed consent form prior to participation in the study. Current protocol version and approval date: IRB-24-0209, amendment 2 (January 4, 2024). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Carson EA. Mortality in state and federal prisons: 2001–2019 Statistical tables. Bureau of Justice Statistics; 2021. https://bjs.ojp.gov/content/pub/pdf/msfp0119st.pdf. Accessed 18 Mar 2024.
-
- Lupez EL, Woolhandler S, Himmelstein DU, Hawks L, Dickman S, Gaffney A, Bor D, Schrier E, Cai C, Azaroff LS, McCormick D. Health, access to care, and financial barriers to care among people incarcerated in US prisons. JAMA Intern Med. 2024;184(10):1176–84. 10.1001/jamainternmed.2024.3567. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
