

ACL repair vs. reconstruction: a meta-analysis of outcomes across different tear characteristics
- PMID: 40764551
- PMCID: PMC12323060
- DOI: 10.1186/s12893-025-03101-6
ACL repair vs. reconstruction: a meta-analysis of outcomes across different tear characteristics
Abstract
Background: Anterior cruciate ligament (ACL) reconstruction remains the gold standard but carries donor-site morbidity and prolonged recovery. Modern ACL repair techniques theoretically preserve native proprioception and enable faster rehabilitation. We hypothesized that modern ACL repair would demonstrate non-inferior clinical outcomes compared to reconstruction.This meta-analysis compares clinical outcomes of primary repair versus autograft reconstruction.
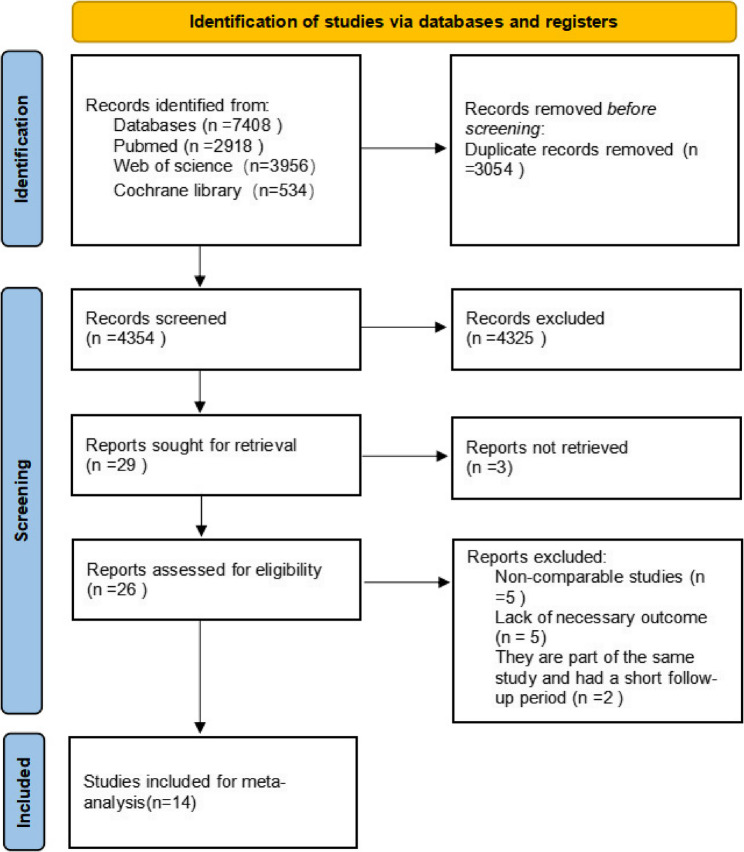
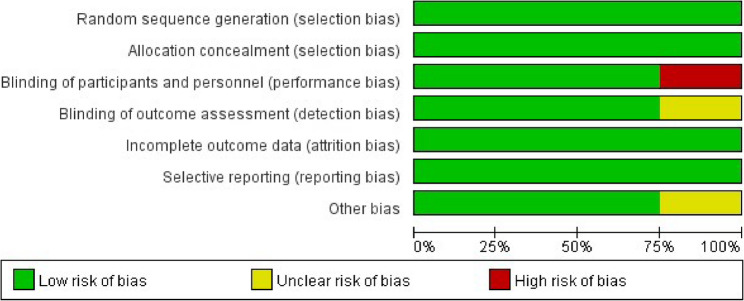
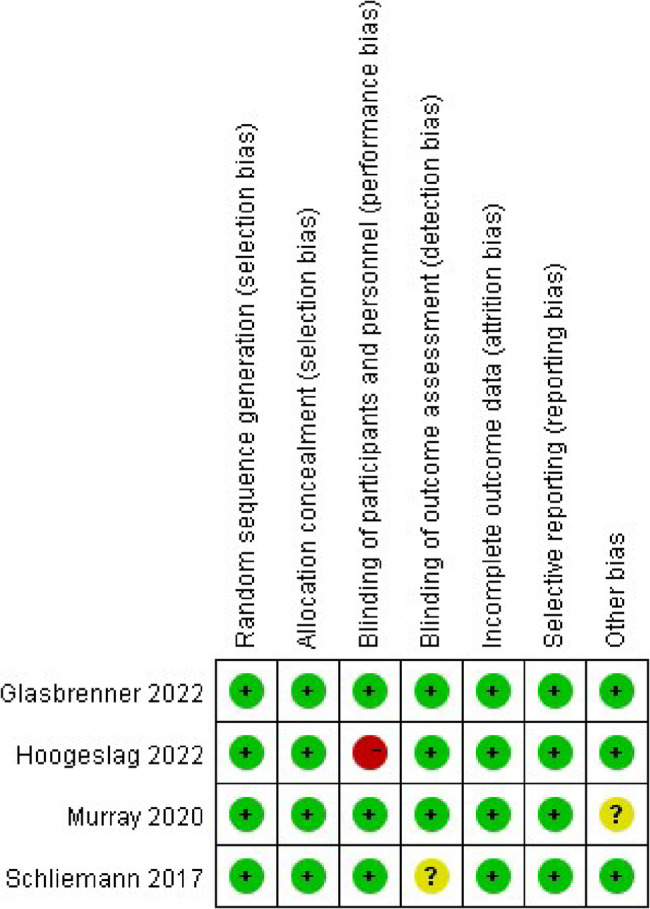
Methods: We systematically searched PubMed, Cochrane Library, and Web of Science (2015–2025) for comparative studies (RCTs, cohorts, case-controls) reporting ≥ 2 key outcomes (failure rate, AP knee laxity, IKDC, Lysholm, or Tegner scores) with ≥ 1-year follow-up. Pooled ORs and WMDs with 95% CIs were calculated using RevMan 5.4. Subgroup analyses (injury-to-surgery time, injury location, study design, repair technique) and GRADE assessment were performed.
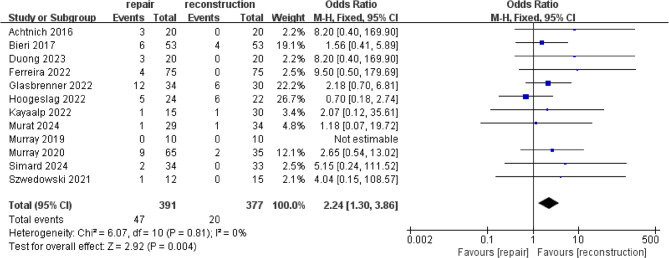
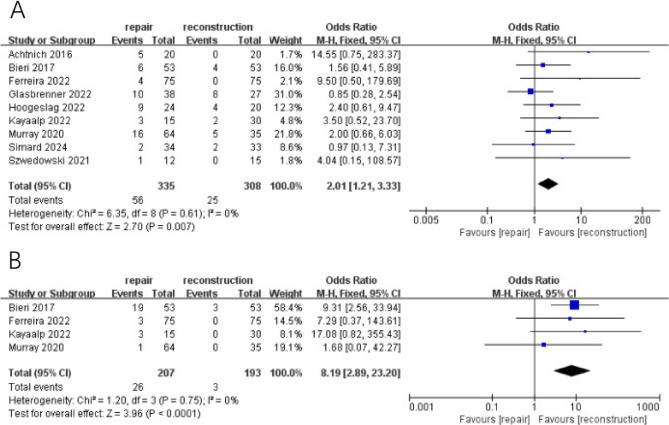
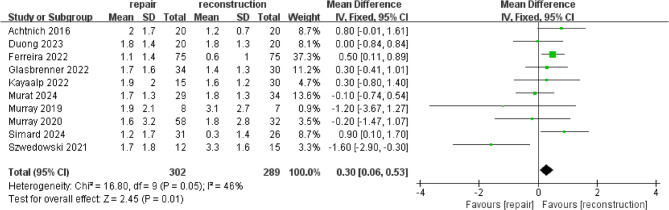
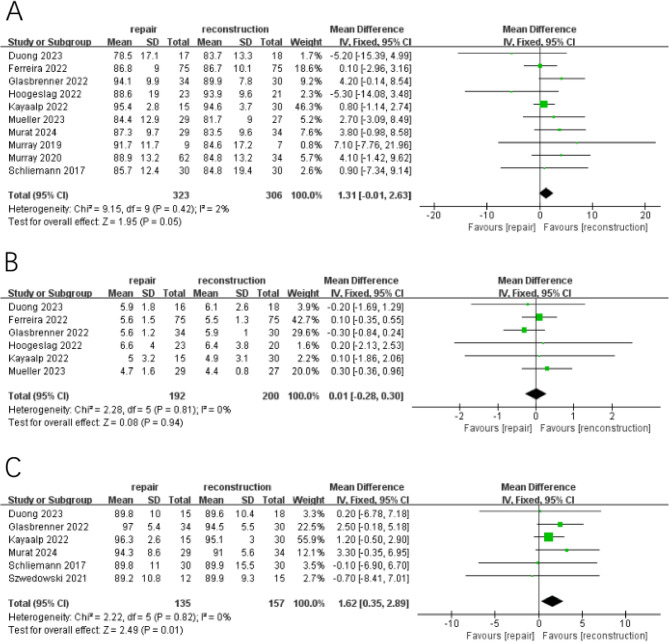
Results: Fourteen studies (4 RCTs, 8 cohorts, 2 case-controls; n = 908 patients) were included (repair: n = 460; reconstruction: n = 448). Failure/Revision Rates: Repair demonstrated numerically higher failure rates (OR = 2.24, 95% CI 1.30–3.86, P = 0.004) and revision rates (OR = 2.01, 95% CI 1.21–3.33, P = 0.007) versus reconstruction.Hardware removal: increased hardware removal incidence was observed in repair groups (OR = 8.19, 95% CI 2.89–23.20, P < 0.001).AP knee laxity: reconstruction showed marginally lower AP knee laxity (WMD = 0.30, 95% CI 0.06–0.53, P = 0.01).Patient-reported outcomes: no significant differences in IKDC (WMD = 1.31,95%CI: −0.01–2.63;P = 0.05) or Tegner scores (WMD: 0.01; 95% CI: -0.28– 0.30;P = 0.94). Lysholm scores slightly favored reconstruction (WMD = 1.62,; 95% CI: 0.35–2.89;P = 0.01).Key subgroup findings: repair achieved comparable outcomes to reconstruction in: (1) RCT-designed studies, (2) Acute repairs (< 21 days post-injury).
Conclusions: ACL repair is associated with higher failure and revision rates than reconstruction overall, but may be a viable alternative in selected patients with acute proximal tears.
Supplementary Information: The online version contains supplementary material available at 10.1186/s12893-025-03101-6.
Keywords: Acute proximal injury; Anterior cruciate ligament; Meta-analysis; Reconstruction; Repair.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: not applicable. Consent for publication: not applicable. Competing interests: The authors declare no competing interests.
Figures
References
Grants and funding
- TSYC202301B077/the Natural Science Foundation of Xinjiang Uygur Autonomous Region
- TSYC202301B077/the Natural Science Foundation of Xinjiang Uygur Autonomous Region
- TSYC202301B077/the Natural Science Foundation of Xinjiang Uygur Autonomous Region
- TSYC202301B077/the Natural Science Foundation of Xinjiang Uygur Autonomous Region
- TSYC202301B077/the Natural Science Foundation of Xinjiang Uygur Autonomous Region
LinkOut - more resources
Full Text Sources
