

Inpatient outcomes among children with Down syndrome: a Kids' Inpatient Database study
- PMID: 40764555
- PMCID: PMC12326621
- DOI: 10.1186/s12887-025-05899-9
Inpatient outcomes among children with Down syndrome: a Kids' Inpatient Database study
Abstract
Background: Children with Down Syndrome (DS) are more likely to have multi-system comorbidities leading to more frequent hospitalizations than the general population. We aim to evaluate whether racial differences contribute to hospitalization outcomes and mortality among children with DS.
Methods: Hospital discharge records were obtained for children (< 21 y) with DS hospitalized between 2006 and 2019 from the Kid's Inpatient Database. The primary exposure was the Black race. Primary outcomes were invasive mechanical ventilation (IMV) and mortality. Secondary outcomes were non-invasive mechanical ventilation (NIMV), length of hospital stay (LOS), and inflation-adjusted cost of hospitalization (IACH). Multivariable logistic regression models were used to ascertain associations between Black race and outcomes.
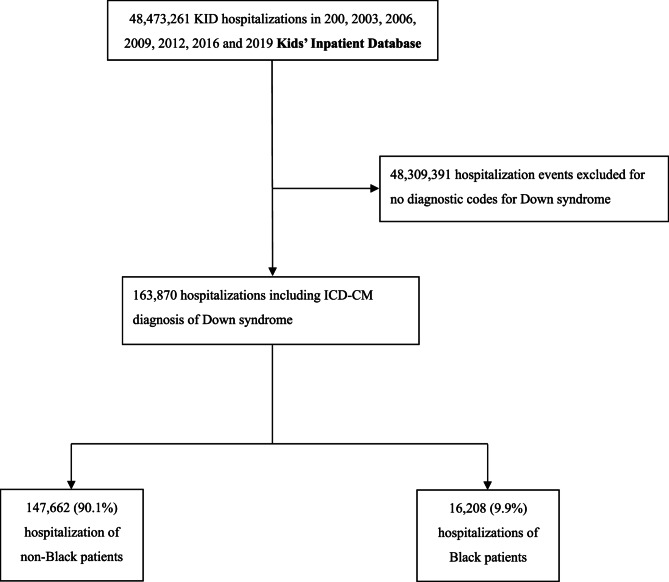
Results: Among 163,870 hospitalizations in children with DS, 16,208 (9.89%) were Black children. Compared with non-Black children, Black children were younger, of lower household incomes, more likely to have public insurance, more likely to have asthma, OSA, obesity, prematurity, congenital heart disease, pulmonary hypertension, congenital airway anomalies, neuromuscular weakness, and dysphagia. Descriptive analyses indicated that Black race was associated with higher risks of mortality, IMV, NIMV, longer LOS, and greater IACH. After multivariable adjustment, Black race remained independently associated with mortality (OR:1.35, 95%-CI:1.15-1.59, p < 0.0001), IMV (OR:1.34, 95%-CI:1.23-1.45, p < 0.0001), NIMV (OR:1.41, 95%-CI:1.26-1.59, p < 0.0001) and increased LOS (IRR:1.08, 95%-CI:1.04-1.13, p < 0.0001), but not IACH.
Conclusions: Hospitalized Black children with DS are more likely to be younger, of lower household incomes, with public insurance, and with other underlying comorbidities. Black children had increased risks of mortality and IMV and increased LOS.
Keywords: Black; Children; Down syndrome.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: KID includes event-level data presented for each admission, and includes diagnostic and procedural codes; the lack of unique identifiers does not allow for identification of repeated admission of the same patients. As all data obtained were deidentified, IRB approval was exempt. Consent for publication: See response in “Ethics approval and consent to participate”. Competing interests: The authors declare no competing interests.
Figures
References
-
- Canfield MA, Honein MA, Yuskiv N, Xing J, Mai CT, Collins JS, Devine O, Petrini J, Ramadhani TA, Hobbs CA, et al. National estimates and race/ethnic-specific variation of selected birth defects in the united states, 1999–2001. Birth Defects Res Clin Mol Teratol. 2006;76(11):747–56. - PubMed
-
- Bull MJ, Trotter T, Santoro SL, Christensen C, Grout RW. Genetics TCO: health supervision for children and adolescents with down syndrome. Pediatrics. 2022;149(5). - PubMed
-
- Leonard S, Bower C, Petterson B, Leonard H. Survival of infants born with down’s syndrome: 1980-96. Paediatr Perinat Epidemiol. 2000;14(2):163–71. - PubMed
-
- Day SM, Strauss DJ, Shavelle RM, Reynolds RJ. Mortality and causes of death in persons with Down syndrome in California. Dev Med Child Neurol. 2005;47(3):171–6. - PubMed
-
- Rasmussen SA, Wong LY, Correa A, Gambrell D, Friedman JM. Survival in infants with Down syndrome, metropolitan Atlanta, 1979–1998. J Pediatr. 2006;148(6):806–12. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
