

Anti-centromere antibody positivity with coexisting idiopathic portal hypertension and primary biliary cholangitis progressing to limited cutaneous systemic sclerosis: a case report
- PMID: 40764937
- PMCID: PMC12326789
- DOI: 10.1186/s13256-025-05426-5
Anti-centromere antibody positivity with coexisting idiopathic portal hypertension and primary biliary cholangitis progressing to limited cutaneous systemic sclerosis: a case report
Abstract
Background: Anti-centromere antibodies are autoantibodies that selectively bind to the centromere region of chromosomes. Studies have indicated that anti-centromere antibodies can induce microvascular alterations and tissue remodeling, ultimately leading to fibrosis. They have been implicated in limited cutaneous systemic sclerosis, including calcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia syndrome, and primary biliary cholangitis, where anti-centromere antibody positivity can be associated with rapid progression of portal hypertension, although the underlying mechanisms remain unclear. Idiopathic portal hypertension, despite being termed "idiopathic," has distinctive pathological, angiographic, and ultrasound findings, and autoimmune processes have been proposed to mediate its intrahepatic microcirculatory disruptions. Interestingly, idiopathic portal hypertension-related small portal vein and scleroderma skin findings share certain similarities. However, no documented cases have linked anti-centromere antibody-induced intrahepatic vascular endothelial dysfunction to idiopathic portal hypertension and subsequent progression to limited cutaneous systemic sclerosis.
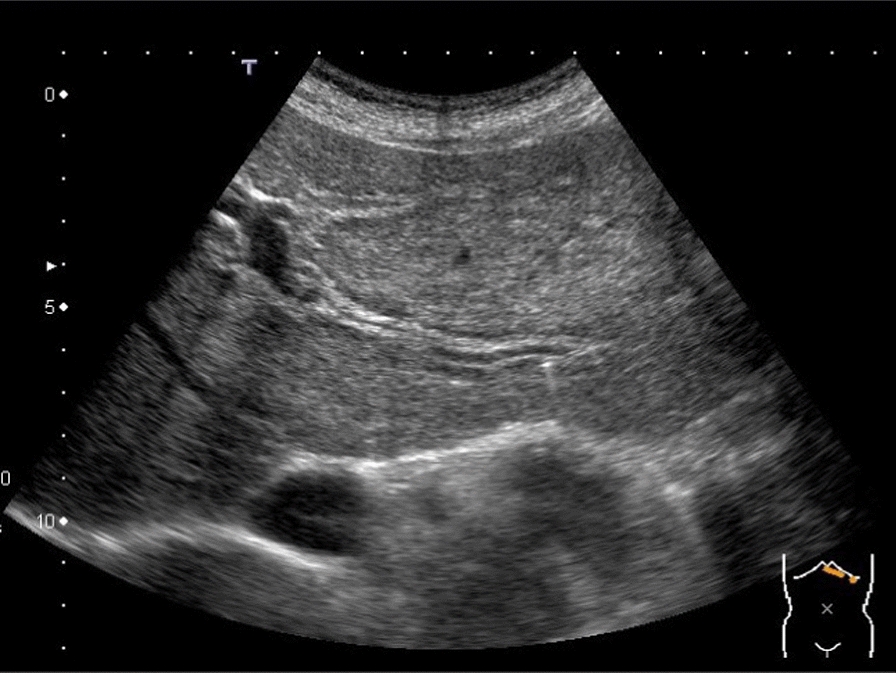
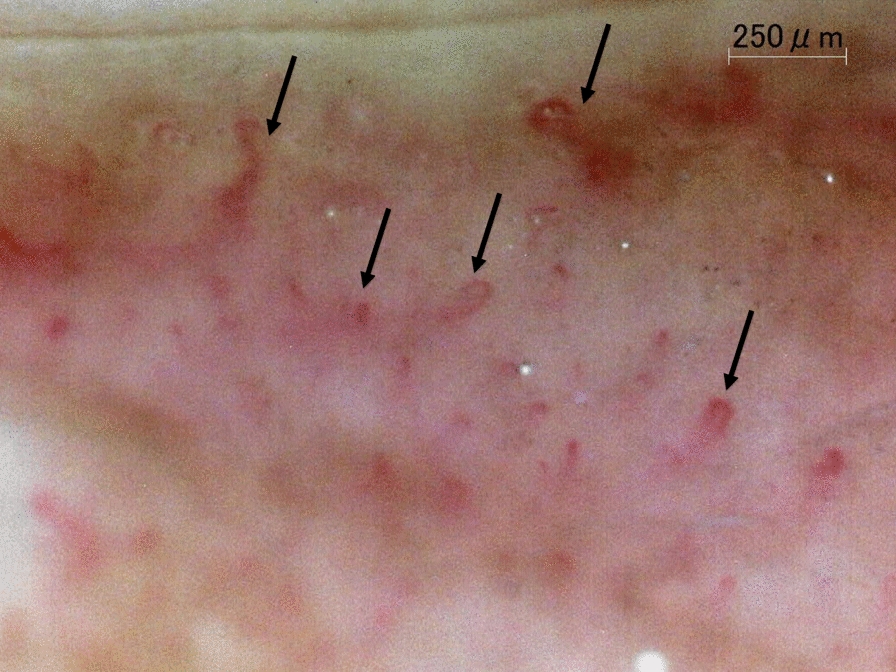
Case presentation: A 57-year-old Japanese woman was referred to our hospital with suspected anti-centromere antibody-positive primary biliary cholangitis. Further examination revealed the coexistence of idiopathic portal hypertension, and the patient progressed to limited cutaneous systemic sclerosis over 3 years. On the basis of this case, we suspected that anti-centromere antibodies might cause microvascular endothelial dysfunction, leading to the development of idiopathic portal hypertension and other systemic abnormalities. Supplementary tests were performed to verify this hypothesis, including flow-mediated vasodilation, brachial-ankle pulse wave velocity, nailfold video capillaroscopy, upper gastrointestinal endoscopy, pathological CD34 and indoleamine 2,3-dioxygenase 1 staining, and measurements of soluble lectin-like oxidized low-density lipoprotein receptor-1 and its ligand containing apolipoprotein B. The results indicated vascular abnormalities in the liver, skin, and gastrointestinal tract, highlighting the universal effects of anti-centromere antibodies in vascular and autoimmune pathologies.
Conclusion: This is the first documented case of hepatic and systemic microvascular impairment observed in an anti-centromere antibody-positive patient. The pathological evidence of endothelial damage in the liver suggests that the "idiopathic" label of idiopathic portal hypertension may need reconsideration in the context of anti-centromere antibody-related pathophysiology, potentially warranting a unifying concept such as "anti-centromere antibody-related systemic microangiopathy syndrome." While our case may provide novel insights into anti-centromere antibody-driven microvascular dysfunction across multiple organ systems, the findings are preliminary. Future studies involving larger cohorts and detailed mechanistic analyses are necessary to confirm the systemic and hepatic effects of anti-centromere antibodies.
Keywords: Anti-centromere antibody; CREST syndrome; Idiopathic portal hypertension; Intrapapillary capillary loop; Liver cirrhosis; Nail capillary microscopy; Primary biliary cholangitis; Vascular endothelial dysfunction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Competing interests: The authors declare that they have no competing interests.
Figures







References
-
- Ahmed SS, Tan FK, Arnett FC, Jin L, Geng YJ. Induction of apoptosis and fibrillin 1 expression in human dermal endothelial cells by scleroderma sera containing anti-endothelial cell antibodies. Arthritis Rheum. 2006;54:2250–62. - PubMed
-
- Corallo C, Cheleschi S, Cutolo M, Soldano S, Fioravanti A, Volpi N, et al. Antibodies against specific extractable nuclear antigens (ENAs) as diagnostic and prognostic tools and inducers of a profibrotic phenotype in cultured human skin fibroblasts: are they functional? Arthritis Res Ther. 2019;21:152. - PMC - PubMed
-
- Nakamura M, Kondo H, Mori T, Komori A, Matsuyama M, Ito M, et al. Anti-gp210 and anti-centromere antibodies are different risk factors for the progression of primary biliary cirrhosis. Hepatology. 2007;45:118–27. - PubMed
-
- The Japan Society for Portal Hypertension. General rules for the study of portal hypertension. 4th ed. Tokyo: Kanehara; 2022.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
