

Assessment of the urinary uric acid-to-creatinine ratio as a diagnostic marker for perinatal asphyxia in a resource-poor setting: a case control study
- PMID: 40764981
- PMCID: PMC12323170
- DOI: 10.1186/s12887-025-05981-2
Assessment of the urinary uric acid-to-creatinine ratio as a diagnostic marker for perinatal asphyxia in a resource-poor setting: a case control study
Abstract
Background: The lack of simple but effective and affordable diagnostic tools presents a challenge for the management of perinatal asphyxia, especially in low- to middle-income countries. Current diagnostic tools, such as arterial blood gas estimation, are expensive and not readily available at primary and secondary levels of care, where most cases of perinatal asphyxia are identified. This causes a delay in diagnosis. Perinatal asphyxia may have improved outcomes if there are cheaper, reliable, and more convenient diagnostic biomarkers that can aid early diagnosis leading to early initiation of treatment. This study assessed the utility of the urinary uric acid-to-urinary creatinine (UUA/UC) ratio in the diagnosis of perinatal asphyxia.
Methods: This study was conducted among 90 term newborns aged less than 24-hours delivered at delivered at the Enugu State University Teaching Hospital (ESUTH). In the study population, there were an equal number of asphyxiated and apparently healthy babies. Relevant maternal and neonatal histories were obtained, and physical examination was carried out for all enrolled newborns. Umbilical arterial blood was collected for blood gas analysis, and spot urine samples were collected and sent for uric acid and creatinine estimation. Relevant statistical tests were applied in the data analysis.
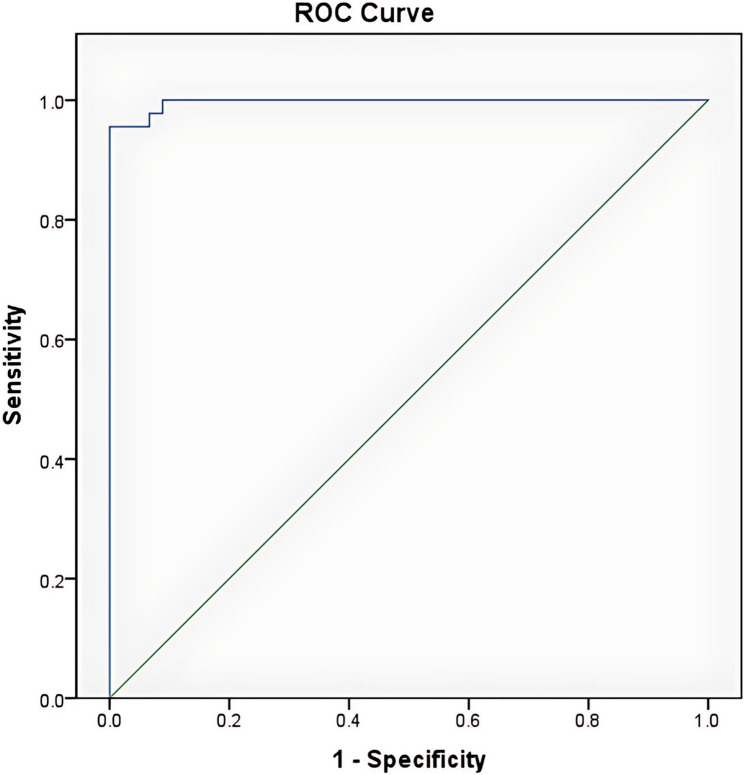
Results: The mean UUA/UC ratio was significantly greater in the asphyxiated group (2.41 ± 0.73) than among the control group (0.87 ± 0.29) (t = 13.129, p < 0.001). The accuracy of the UUA/UC ratio in diagnosing perinatal asphyxia had an area under the curve (AUC) of 0.978, implying that the test is accurate. The cut-off point that gives the best diagnosis of perinatal asphyxia was 1.54, with a sensitivity of 95.6%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 96%. Additionally, the UUA/UC ratio has a very strong positive correlation with the severity of hypoxic-ischaemic encephalopathy (HIE) (r = 0.843, p < 0.001).
Conclusion: The UUA/UC ratio is a good diagnostic marker of asphyxia and varies with the severity of encephalopathy. Accordingly, the urinary uric acid-to-creatinine ratio is recommended as a surrogate biomarker for the diagnosis of perinatal asphyxia.
Keywords: Creatinine; Diagnosis; Perinatal asphyxia; Urinary uric acid.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for the study was obtained before the commencement of the study from the Ethics and Research Committee of the ESUT Teaching Hospital, Parklane, Enugu, with reference number ESUTHP/C-MAC/RA/034/Vol.1/291. Written consent was obtained from the parents or legal guardians of the neonates after the details of the research, including the specimen collection, had been explained. The study was conducted in accordance with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Ekwochi U, Asinobi NI, Osuorah CDI, Ndu IK, Ifediora C, Amadi OF et al. Incidence and Predictors of Mortality Among Newborns With Perinatal Asphyxia: A 4-Year Prospective Study of Newborns Delivered in Health Care Facilities in Enugu, South-East Nigeria. Clin Med Insights Pediatr [Internet]. 2017;11:117955651774664. Available from: http://journals.sagepub.com/10.1177/1179556517746646 - PMC - PubMed
-
- Antonucci R, Porcella A, Pilloni MD. Perinatal asphyxia in the term newborn. J Pediatr Neonatal Individ Med. 2014 [Cited 11 Oct 2018];3(2). Available from: www.jpnim.com. Accessed 2018 Aug 25.
-
- Malta DC, Duarte EC, Escalante JJC, de Almeida MF, Sardinha LMV, Macário EM, Monteiro RA, Neto OLM. Avoidable causes of infant mortality in brazil, 1997–2006: contribution to performance evaluation of the united National health system. Cad Saude Publica. 2010;26(3):481–91. - PubMed
-
- Mehta A, Chawla D, Kaur J, Mahajan V, Guglani V. Salivary lactate dehydrogenase levels can provide early diagnosis of hypoxic-ischaemic encephalopathy in neonates with birth asphyxia. Acta Paediatr. 2015;104(6):236–40. - PubMed
-
- Zhang XH, Zhang BL, Guo SM, Wang P, Yang JW. Clinical significance of dynamic measurements of seric TNF-α, HMGBl, and NSE levels and aEEG monitoring in neonatal asphyxia. Eur Rev Med Pharmacol Sci. 2017;21(19):4333–9. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
